On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
SYNESTHESIA
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
14. Changing Conception of Autism

Today we know autism is a neurodevelopmental condition that affects individuals differently, with widely varying symptoms and levels of impairment. This includes difficulty processing information. Learning issues, communications issues, difficulties engaging with others at events, play, work. The modern version of autism was based on groundbreaking work from the late 1970s, when science was learning how the brain works and how children’s brains develop.
Autistic individuals were diagnosed very early in life, with most symptoms showing up by age 2. These babies grow up understanding their autism. Others diagnosed later in childhood or even into adulthood reshape their self-perception — often appreciating new insights into why they’ve felt different for so long.
In this post, I’ll continue the history of autism, from the triad of impairments (DSM-4) to autism as a spectrum disorder (DSM-5).
Triad of Impairments
In 1979, British psychiatrists Lorna Wing (cofounder, UK’s National Autistic Society) and Judith Gould found autism prevalence among children with special needs (IQ under 70) to be 5/10,000. In 1986, Wing and Gould found a larger group of children—15/10,000. Based on their observations and study, they developed the concept of what they called the triad of impairments, to better understand the challenges facing them.
- Social interaction, in understanding/interpreting social rules, behavior, and relationships, seeming indifferent to others, not understanding taking turns, engaging in reciprocal conversation, and maintaining eye contact.
- Social communication, in both verbal and non-verbal communication, ranging from delayed or limited speech to nonverbal. Those with verbal abilities may struggle with pragmatic language skills, such as understanding sarcasm or using appropriate tone of voice. Others may also not fully understand nonverbal communication, including common gestures and facial expressions.
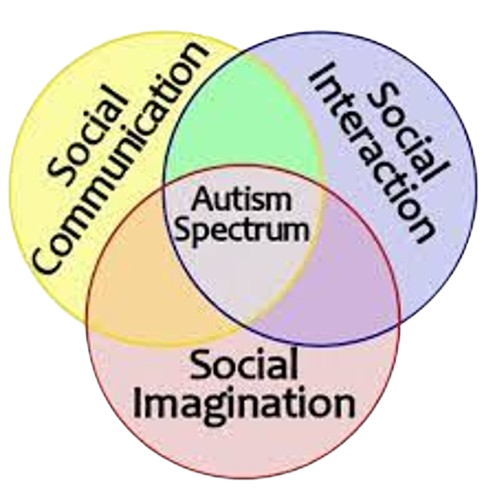
Graphic: “The Triad of Impairments and Other Autism Myths,” Psychology Network
- Restricted and repetitive behaviors (RRBs), including “stereotyped” patterns of activities or repetitive movements, like hand flapping, finger tapping, rocking, or something harmful like head banging. They may show an intense interest in a specific topic, adhere to obsessively strict routines, obsessively follow rituals, and have severe sensory sensitivities, limited interpersonal play, and imagination.
The triad was used as the common denominator of separate autistic subtypes appearing in the 1994 Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-4). In DSM-5, published in 2013, the triad was changed to a dyad of impairments. Social and communication deficits are merged as one, because they’re seen as inseparable. It means individuals with autism primarily struggle with interacting socially and exhibit repetitive patterns of behavior.
In newer thinking, the shift from behaviors to underlying cognition is likely to see more revisions. A recent paper, “The triad of impairment in autism revisited,” by Andrew Cashin, et al., PubMed/NIH, described the original role of the triad of impairment as shaping understanding of autism and guiding support and intervention strategies—allowing professionals and families to share a common language and relate to those with autism. But the authors note how understanding has moved well beyond this picture of autism.
Like the evolution of many concepts, this was a transitional idea. The original triad of impairments described the behavioral manifestation; the actual triad of impairments is at the level of cognitive processing. The actual triad of impairment is static and ubiquitous, unlike the variable and fluctuating behavioral manifestation. The actual triad of impairment in autism is visual as opposed to linguistic processing, impaired abstraction, and lack of theory of mind. The actual triad is central to all diagnoses that together makes up the autism spectrum. — Andrew Cashin, et al., “The triad of impairment in autism revisited,” PubMed/NIH
Autism Prevalence: Recent
In 2020, according to the Center for Disease Control and Prevention’s (CDC’s) Autism and Developmental Disabilities Monitoring (ADDM) Network, individuals of all genders, races, ethnicities, and economic backgrounds can have autism. ADDM data shows autism frequency surging over the past 20 years, which shows up differently in White and Black children. It’s not clear whether autism is increasing, whether experts are more aware of it, or whether diagnoses encompass more people with less impairment. Data points:
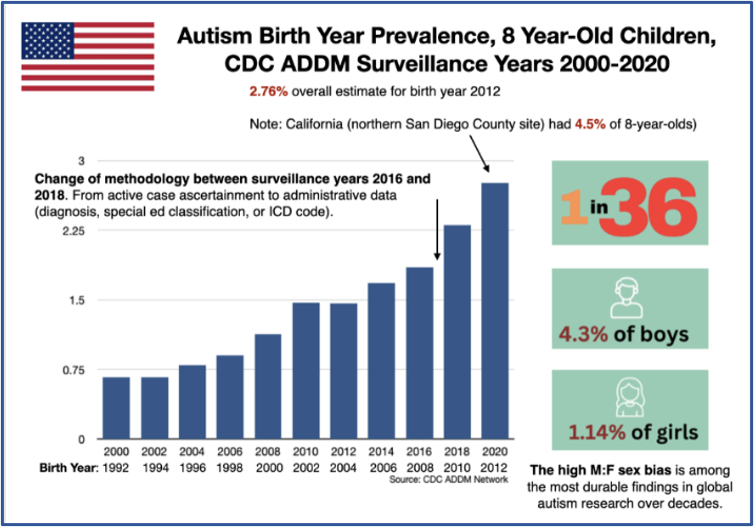
Source: “Getting Real About Autism’s Exponential Explosion,” National Council on Severe Autism
Source: Vaccine Evidence
- Autism in children: 1/36 8-year-olds (4% boys, 1% girls) were estimated to have autism — higher than 2000-2018 ADDM Network.
- Gender: Boys are 4X more likely than girls to develop autism. Yet girls and women are often overlooked and misdiagnosed.
- Racial/ethnic: For the first time in 8-year-olds, racial/ethnic groups increased, reversing a trend. Black children were also more likely than White children — both with autism — to have intellectual disability.
- Co-occurring conditions: About 1/6 (17%) of 3–17 year olds were reported by parents as having a developmental disability: autism, ADHD, blindness, cerebral palsy. Epilepsy affects 30% of autistic children.
- Age: Average age of autism diagnosis is 4–5 years. In most instances, infants develop normally at first and then regress, at 18-24 months, losing language and motor control.
- Education: Nearly 74% of U.S.autistic students graduate high school.
Public Health Action: Need to Focus on Diversity
In “The Future of Autism Treatment,” Children’s Hospital of Los Angeles (CHLA), writer Ellin Kavanagh notes increases of children identified with autism—particularly non-White children and girls. She quotes Shafali Jeste, who in 2022 moved her research lab, Kids with Neurogenetic and Developmental Disabilities (KiNDD), to CHLA to reach a more diverse population:
Families of other ethnicities and socioeconomic status typically don’t participate in research…. We have done a poor job of introducing these studies to families from under-represented minority groups and those with low incomes… There are some real barriers to participation in studies, especially cost and time. —Physician Shafali Jeste, quoted by Ellin Kavanagh, “Future of Autism Treatment,” Children’s Hospital of Los Angeles (CHLA)

It’s impossible to understand why autism is rising among low-income Black or Hispanic children through a study of middle-class White children. Jeste’s team, Kavanagh writes, removed “some of those barriers by paying for transportation to the clinic for assessments, providing childcare for siblings, and having evening and weekend appointments.”
Same for genetic testing. Kavanagh notes more clinicians are using advanced genetic testing to identify causes but interpretation relies on large databases that lack diversity.
Physician Bridget Fernandez, medical geneticist/clinical research associate director, CHLA’s Saban Research Institute, says knowledge of genomic changes is based on studies of people of European ancestry. Her database assessing Hispanic children corrects this inequity.
Recognition of Autism Spectrum Disorder (ASD)
- Asperger’s syndrome (see post 13) showed typical autism symptoms — communications/ social problems — but average-to-above average intellect, good language, no cognitive delays, able to handle daily life. Many believe Albert Einstein had this version (see post 18).
- Pervasive developmental disorder-not otherwise specified (PDD-NOS) was milder, with some but not all traits — communications/social impairments and stereotyped/repetitive behavior — on the spectrum between classic autistic disorder and Asperger’s.
- Childhood disintegrative disorder (CDD) — or Heller’s syndrome or disintegrative psychosis — symptoms behave differently neurologically. Children develop normally for 2 years, then aged 2-10 lose language/social/motor skills, with severely changed behavior/mood.
- Rett’s syndrome only occurs in girls. It’s genetic and can be medically confirmed. Babies develop normally up to 6-18 months, then start losing social and communications skills through age 4 — resulting in severe mental and physical disability.
DSM-5 changed ASD from separate disorders into one condition with a “dyad of impairment” (the term was later dropped): (A), social deficits (persistent deficits in social communication or interaction) and (B), restricted behaviors (repetitive patterns of behavior). Symptoms are arrayed on sliding scales of severity, from mild to severe.
According to the University of Oregon’s Autism History Project, removing Asperger’s caused the most controversy around the revision — with potential loss of needed services and absence of diagnostic boundaries. Since then, the psychiatric field has developed measurement tools, now today’s standard for diagnoses. Child Mind Institute describes the Autism Diagnostic Observation Schedule (ADOS-2), with different modules for different ages of children — a play-based version for toddlers or a more conversational module for children ages 3+.
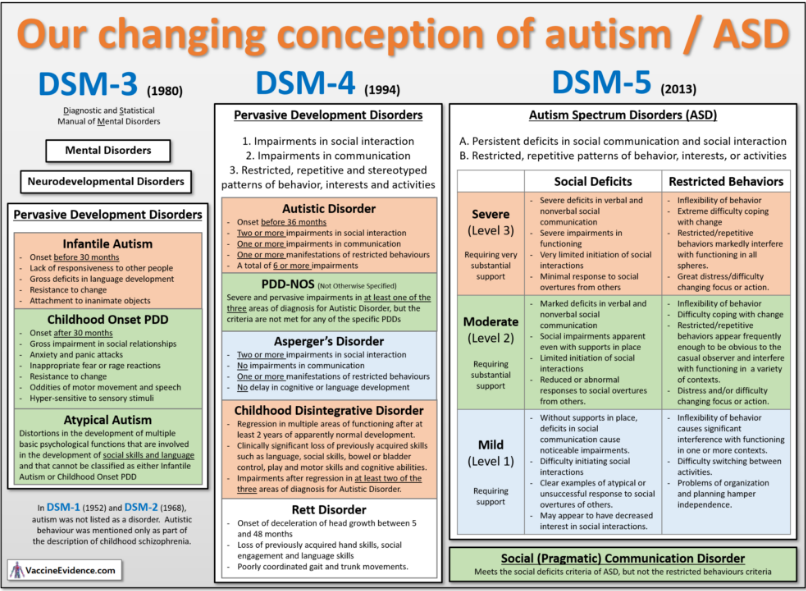
Source: Vaccine Evidence
The Deep Bias of DSM-5 Criteria
These changes might seem hair-splitting, until you read a provocative Medium post, “A Neurodiversity Paradigm Breakdown of the DSM-5 Criteria for Autism,” by autistic trauma specialist, researcher, writer, and neurodiversity advocate Janae Elisabeth. Elisabeth sees DSM-5 as “a speculative story from a dominant cultural group about a minority cultural group presented with deep bias and without any attempt to understand how that minority cultural group perceives their differences.” She cautions her readers this way:
The medical model of autism presented in the DSM may be particularly disturbing for autistics to read. If you begin to feel dysregulated, it’s ok to stop and come back to this later when you’re feeling more resourced. —“Trauma Geek” Janae Elisabeth, Medium
Elizabeth writes, “… a child must have: (A) persistent deficits in each of three areas of social communication and interaction, plus (B) at least two of four types of restricted, repetitive behaviors.”
In respect to (A), DSM-5 states: “Deficits in social-emotional reciprocity, ranging from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.”
All of these apparent “deficits” are either stress or trauma responses or perfectly functional neurodivergent social interactions. A stressed or traumatized autistic person will not feel safe to hold conversation, share interests, or initiate social interactions because of the trauma associated with past attempts.
In addition, the expectation of back-and-forth conversation, sharing of emotions, and initiating social interaction is uniquely neurotypical. Autistic people do not need to speak to share emotional information, we have different cultural conversation patterns, and we often prefer to let others initiate socialization so that we can be sure they are participating willingly. —“Trauma Geek” Janae Elisabeth, Medium
I won’t recount Elizabeth’s long, detailed response to (B). But her commentary was an eye-opening caution for any neurotypical (NT) writing about neurodivergent (ND) conditions and experiences. As someone who places a lot of faith in medical literature and research, I must reread my sources with humility and care for positions not recognized nor accounted for.
The neurodiversity movement was born at the moment when the NT community decided what was best for the ND community without their involvement. For this and many other reasons, I will no longer use autism spectrum disorder or ASD in my writing—except for in this post. Disorder is out, on the spectrum is okay. I’ve also noticed that those with autism are fine with it as a standalone term and as an adjective. If they call themselves autistic, I will, too.
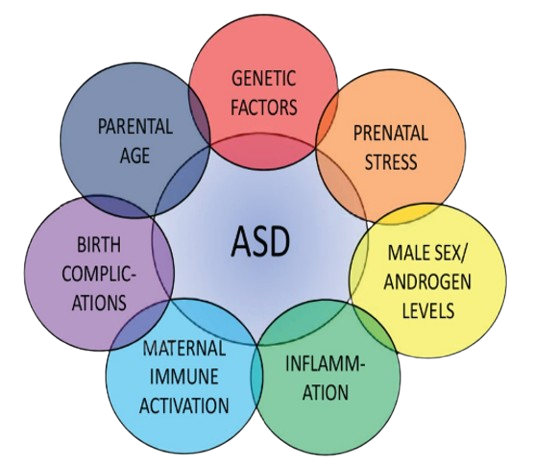
Risk Factors and Causes
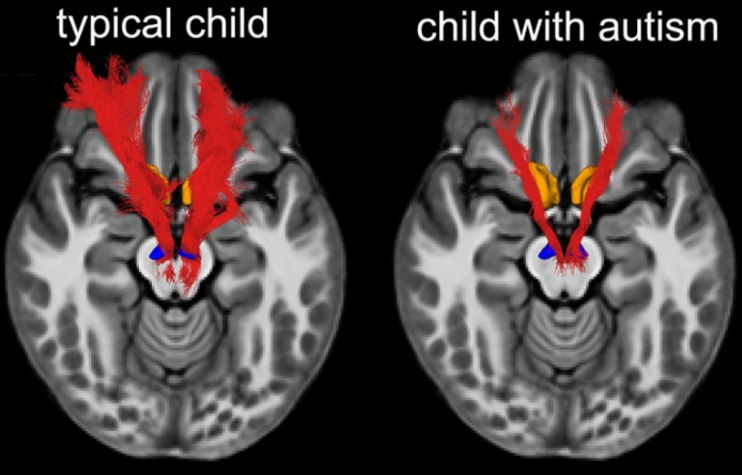
MRI scans reveal children with autism have deficits in a brain pathway that typically makes social interaction feel rewarding. Nerve-fiber tracts along the pathway, in red, are less dense in children with autism than in typically developing children. Kaustubh Supekar, Stanford Medicine
Autism is acknowledged as complex and likely to have several probable risk factors:
Genetics: Recent research indicates 40%-80% of autism risk is genetic, with more than 200 specific genes linked to the disorder. Other data points:
- 15% of children with autism have other genetic disorders, which can cause developmental delays, intellectual disabilities, and mood disorders.
- Other genes may affect brain development, severity of symptoms, or how brain cells communicate. These can include: fragile X syndrome, tuberous sclerosis, Down syndrome.
- Some chromosomal abnormalities and single gene mutations are inherited, and others occur spontaneously.
- According to the National Fragile X Foundation, 20% of younger siblings of a child with autism also have autism—much higher than CDC-reported 1%-2% risk in general population.
- Parents or relatives might have minor problems with social or communication skills themselves or engage in certain autistic behaviors.
- Autism may connect with being born to older parents, but more research is necessary.
Graphic: Transmitter
Behavioral characteristics: Those with autism are often comorbid with attention-deficit/hyperactivity disorder (ADHD), social anxiety disorder (SAD), and sensory processing disorders (SPD).
Environmental factors. Researchers are exploring whether non-genetic factors trigger autism:
- Birth complications, like extreme prematurity, low birth weight, oxygen deprivation to baby’s brain
- Maternal obesity, diabetes, immune system disorders
- Medication
- Viral infections or prenatal exposure to air pollution or certain pesticides
No evidence links autism and child vaccines: The original study igniting debate was retracted due to poor design and methodology. This unproven risk factor continues to persist.
In Sum
Graphic: “Top Companies in Autism Spectrum Disorder Market,” LinkedIn
Both NT and ND individuals process information, learn, interact/ communicate with others, and participate in daily activities. But they may do this differently in their differently wired brains. Common symptoms across the autism spectrum are restricted interests and stimming or repetitive patterns of behaviors. Autistic people can experience sensitivity or discomfort from sensory stimulation, like certain lights or sounds, or from overloaded sensory stimulation. It also seems that DSM-5 needs another round of revision.
Let’s hope by DSM-6, they figure out what’s needed is the professional and research communities absorb the lessons of the neurodiversity movement and make sure to:
- Represent diverse populations in research studies and clinical trials.
- Include people with autism as contributors to research design and feedback.
- Give full consideration to what symptoms are a reaction to NT discrimination and stigma and what are truly neurological impairments that require supports and services.
- Allow people with autism full access to independent living, so they can claim their grace and humanity.
Coming Up Next
In the next posts, I’ll talk about the risk-benefits of diagnoses for a ND condition that advocates argue should no longer be viewed as a disorder, but as a neurological condition deserving support, accommodations, social acceptance, and opportunity. I’ll continue referring to symptoms recognized in DSM-5, as the current go-to resource for professionals. I start with Post 15. Autism Diagnoses and Behavior Patterns, covering early diagnosis and symptoms.
Sources
Copyright ©2026 Jan Swan