On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
20. ADHD and Neurodevelopmental Disorders

Photo: iStock by Getty Images
When my sons were diagnosed with ADD as boys, I thought it was a mild attentional problem showing up mostly around homework. I minimized it back then, as I’ll talk about later, but sure don’t now. ADHD is the reason I’ve devoted myself to this ever-expanding series on neurodivergence. Neurodivergence is closely connected to neurodevelopmental conditions and challenges, but also to ones that are acquired in life, due to trauma, illness, or accidents. Since there’s a confusing array of words beginning with neuro-, I’ll start this post with definitions.
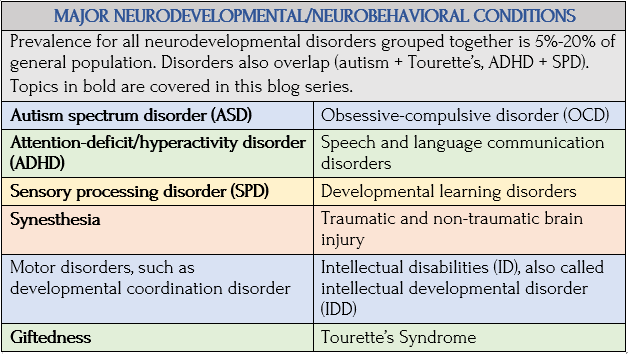
Neurodevelopmental and Neurobehavioral
Researcher Dilip Patel, et al., write, in “Neurodevelopmental and Neurobehavioral Disorders,” PubMedCentral/NIH, the two terms are interchangeable with overlapping characteristics. Neurodevelopmental disorders affect behavior, emotions, and learning processes, especially in children whose developing brains and growing bodies are on a parallel track.
Clinicians refer to this as the developmental period—infancy through adolescence—often with lifelong conditions. Patel, et al., note some prefer neurodevelopmental disabilities “to define chronic disorders that affect central nervous system function during the developmental period, in domains of motor skills, cognition, communication and/or behavior.”
Very Well Mind uses neurobehavioral to define disorders involving brain impairment, injury, or disease, which don’t develop but happen. Brain damage caused by a blow to the head (traumatic brain injury/TBI) or by dementia or multiple sclerosis (non-traumatic brain injury/NTBI). “These disorders are characterized by significant, observable behavioral changes in the people who develop them.” New news reports TBIs cause life-long brain damage.
The World Health Organization (WHO) defines neurodevelopmental disorders as “behavioral and cognitive disorders that arise during the developmental period” that involve significant difficulties in acquiring/executing intellectual, motor, or social functions.”
These complex disorders are “presumed to be primarily due to genetic or other factors present from birth.” WHO notes other contributing factors are a lack of appropriate environmental stimulation and learning experiences, disorders arising from injury, disease, or “other insult to the central nervous system, when this occurs during the developmental period.”
DSM criteria shows the range of developmental deficits, from “specific limitations of learning or control of executive functions to global impairments of social skills or intelligence.”

Photo: iStock by Getty Images
Source: World Health Organization
The Neurodevelopmentally Neurodivergent
Autism and other neurodevelopmental disorders have similar trajectories:
- Early childhood onset
- Broad spectrum of severity (low-to-high functioning)
- Broad spectrum of comorbidities (co-occurring, like ADHD+bipolar)
- Symptoms challenging fit in a world created by/for neurotypicals
Neurocognitive Mechanisms in the ADHD Brain
Source: Wikipedia
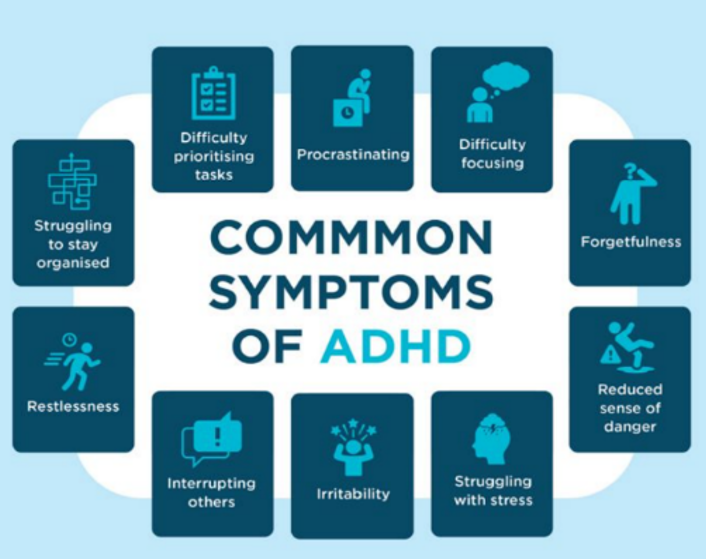
According to Wikipedia, ADHD’s a complex “neuropsychiatric condition with developmentally inappropriate” levels of inattention and hyperactivity/impulsivity—which rarely occurs in isolation. Most people experience other problems, like aggression, academic failure, or interpersonal difficulties. The ADHD brain has degrees of impairment of its neurocognitive mechanisms—combining neural dysfunctions and cognitive deficits—specifically, impaired cognitive control (more popularly known as executive function/EF).
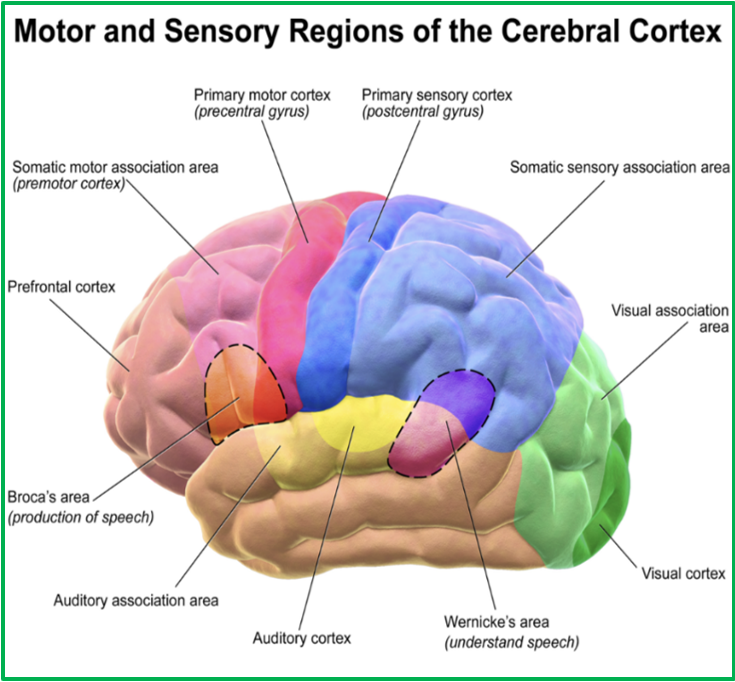
Within our central nervous system (CNS) resides the profoundly busy prefrontal cortex (PFC), the last part of our brain to evolve (as in evolution) and the last part to mature (sometimes not until ages 27-30). The PFC is our “personality center”—what makes us people. It’s where all our cognitive processing takes place, where we mix unconscious sensory stimuli with conscious thought, compare what’s happening with prior experiences, project into future aspirations, and then feel, think, react.
The neurocognitive system, with its complex of neurons, neural pathways, and brain regions, is the biological basis for cognition. It’s complex and awe-inspiring to understand how our cognitive functions, especially cognitive control (executive function/EF), are linked to brain areas and systems that control thought, memory, language, problem-solving, attention, planning, emotions, impulse control, motor control, and all the other features of mind and body.
The ADHD Brain
Source: Wikipedia
If neurocognition is directly responsible for managing emotion, behavior, and movement, what’s the significance for the person with ADHD?
Cognitive control/EF is impaired. Dry science terms describe fascinating brain-centered processes that are affected: stable conflict, inhibitory control (or response inhibition), attention allocation, conflict detection, and working memory.
There’s more. Another thing affecting the ADHD soul are non-EF brain deficits: variable motor timing, variable response speeds, delay aversion, and gross motor problems. This chart give in-brief descriptions:
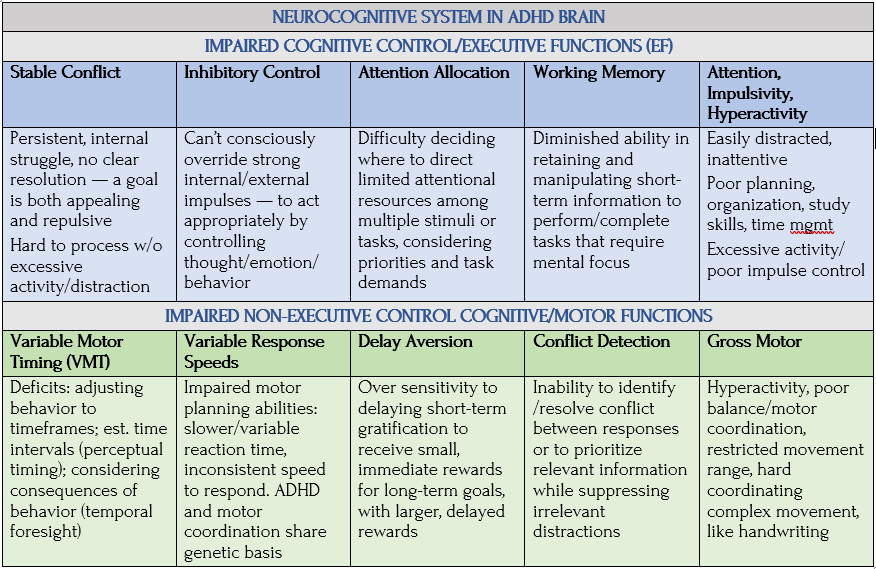
Sources: Wikipedia, PubMed Central/NIH
Crossing from “Normal” to ADHD
ADHD is the most common neurodevelopmental disorder of childhood and adolescence. But where’s the line between “normal” and ADHD?
There are important differences between ADHD brains vs non-ADHD brains. These differences—including those related to brain structure, function, and chemistry—explain many ADHD traits, such as inattention, hyperactivity, and impulsivity. —Jacqueline Sinfield, ADHD coach, author of Untapped Brilliance, How to Reach Your Full Potential As An Adult With ADHD, VeryWellMind
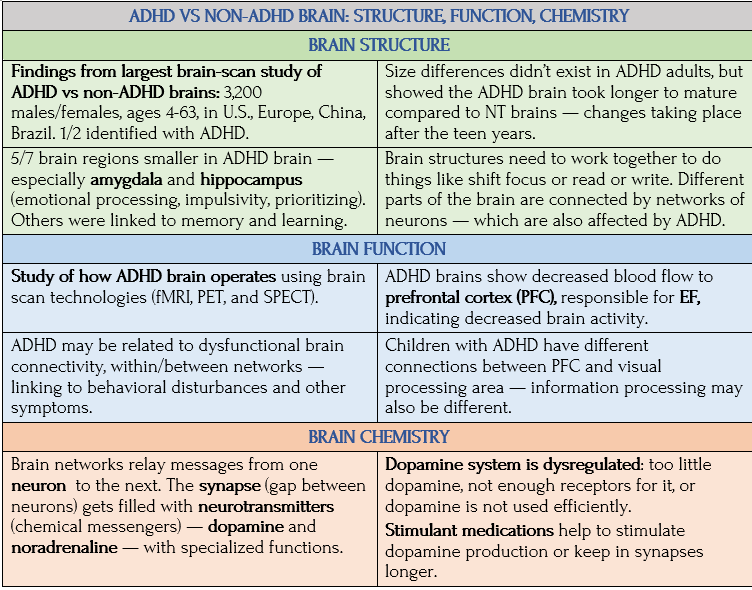
Sources: Jacqueline Sinfield, VeryWellMind. The 2017 brain-scan study was conducted by the ENIGMA consortium, an international group investigating genetic/brain-imaging differences in psychiatric disorders, published in 2017 in The Lancet; funded by National Institutes of Health
In “ADHD and the brain,” Understood, Julie Rawe notes an ADHD brain-scan study shows it’s not only a functional problem, but a brain structure problem, with lags in the brain’s cognitive control/EF system. She writes, “ADHD brain networks have trouble shifting gears.”
Source: Julie Rawe, “ADHD and the brain,” Understood for All, Inc.
Understanding Glutamate Also Matters
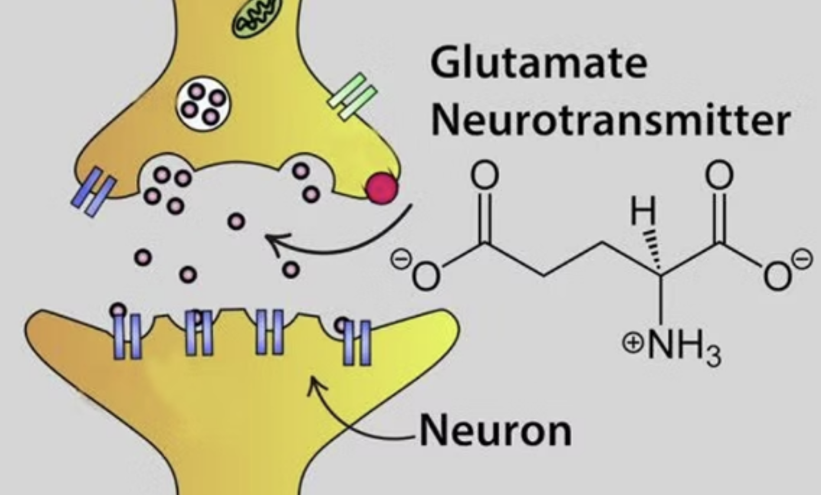
Neuroscience: Neurotransmitters,” Maria McGovern, By Arcadia. Illus: Tran, et al., 2009
In addition to dopamine, which I cover in more depth in the next post, there’s another brain substance that, when imbalanced, shows strong links with ADHD — and autism. It’s glutamate.
Research suggests glutamate imbalances, particularly in the PFC, disrupt signaling pathways to brain functions for attention, focus, and cognitive control — potentially contributing to hyperactivity, impulsivity, and difficulties with social interaction — associated with ADHD and autism. Studies show evidence of altered glutamate levels in ADHD brains. Some indicating a potential hypo-glutamatergic state (lower than typical levels) in certain brain regions — again, contributing to impaired brain function in ADHD. Research has also identified genetic variations related to glutamate receptors associated with increased risk for ADHD/autism.
Dysfunction of glutamate receptors has also been linked to Alzheimer’s disease and migraine headaches. Chronic stress can lead to malfunctioning of the glutamate system, which can impair learning and memory. Glutamate is involved in:
- Learning and memory: Forming new memories and strengthening existing ones
- Cognition: Higher-order processes such as attention, decision-making, problem-solving
- Movement control: Regulates muscle contraction and coordination
- Sensory perception: Modulates perception of taste, smell, and pain
- Mood regulation: Contributes to feelings of happiness, anxiety, and depression
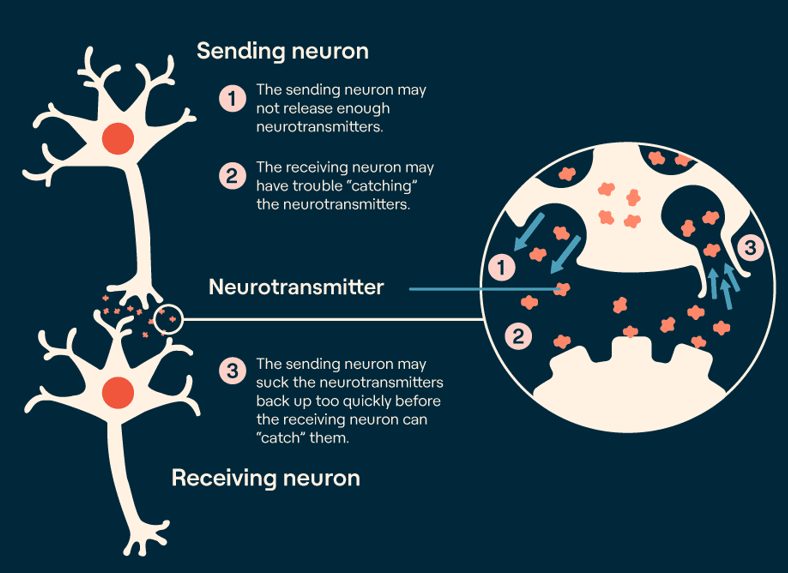
Here’s the science: Glutamate (an amino acid) is the main and plentiful excitatory neuro-transmitter in the central nervous system (CNS), which stimulates neurons to fire, and is vital for cognitive processes like attention and working memory. To carry signals between neurons it needs to attach itself to new cells by binding onto various receptors—most notably to NMDA (N-methyl-D-aspartate) receptors. Glutamate passes calcium into the cells, carrying electrical or chemical signals important for cognitive functions. It’s also found in some foods (cheese, tomatoes, soy sauce), though excessive consumption leads to headaches and other reactions (some might remember MSG in Chinese restaurants). Potential mechanisms:
- Reduced glutamate levels:Research suggests lower glutamate levels in ADHD brains potentially lead to decreased neuronal activity in areas important for attention.
- Impaired glutamate receptor function could also contribute to abnormal signaling.
- Disrupted balance with other neurotransmitters like GABA (which has inhibitory effects) may be disrupted in ADHD, leading to imbalances in brain activity.
Due to the glutamate’s potential role in ADHD and autism, researchers are exploring the development of medications that target the glutamate system as future treatments.
Jaden, Etan, and Chaos Brain

Like most neurotypicals, I was unaware of my intact cognitive control functioning—planning complex projects, organizing my home and my sons’ needs and care, concentrating, meeting deadlines, having reasonable expectations for my future. Except for my ADHD’er sons, I’d still be in that oblivious headspace. Both were diagnosed as children with ADD—a precursor to ADHD. I wasn’t too surprised based on their pre-school delays, a little klutzy on the monkey bars, a little socially shy, and a bit clueless about what school required. I saw them as the future Spock’s, different, but super smart. I had no idea I was about to enter an alternative universe without a star ship.
When the H for hyperactivity entered their diagnoses, I embraced it less about incessant movement, tapping, or disruption and more about chaos in the brain. My calm, sweet little boys didn’t have outwardly “hyperactive” ADHD, but the H was still in there—invisible to parents and teachers. I saw chaos brains as not knowing to place completed homework in the wire basket near the teacher’s desk, losing your viola, in fact losing all gloves and hats, eyeglasses, jackets, T-shirts, many textbooks, and being constitutionally unable to make the bed. I saw chaos brains as global cluelessness about how the world worked. Otherwise, they were “normal.”
Poster Boys for Neurodivergence
Except they weren’t. Jaden and Etan had more than chaos brain. They had serious executive function (EF) and coordination deficits, sensory processing disorder (SPD), generalized anxiety disorder (GAD), social anxiety—and, from all these feelings of not fitting in and other emotional challenges, lifelong trauma. In his mid-20s, Jaden developed bipolar disorder I (see my series on BD), and Etan continues to deal with GAD (see my series on anxiety), SPD, and treatment-resistant depression (TRD).
My sons were poster boys for neurodivergence before the term came to our attention. Today I admire their courage in facing so many obstacles to leading a semi-normal life and certainly lives with financial independence. My challenge has been to understand ND as an NT outsider and by blogging my learning journey. I’m also sharing what I’m learning with them.
Poster by JANLAN, Amazon
Texting: Did you know … ?
- About synesthesia (yes, said Etan, I have that. You do? You never told me!)
- About delay avoidance (yes, said Etan, I have that)
- Bipolar people have less dopamine in their brains (no, I didn’t know, said Jaden — but it makes sense. Good to know there are ways to boost my dopamine levels).
- Ditto with ADHD — not enough dopamine. And ADHD correlating with brain fog (wow, wrote Etan, the article you sent is about me).
- High correlation between bipolar and ADHD (I didn’t know, said Jaden. [Unfortunately, he’s untreated for ADHD, because stimulants trigger mania.])
More from Etan, Age 34
From my formative years, I felt inferior and incapable of dealing with life. I’ve always feared what would come next. I still do. Other people go step by step. But for me, it’s not a stairway. It’s a bunch of shifting steppingstones across a pond or Hogwarts’ stairways.
Depression is comorbid with ADHD a lot of the time, but anxiety big time. My depression is maybe more clinical because it’s consistently there regardless of my situation. If I don’t deal with it, it gets worse. It’s an unfortunate cocktail of clinical depression, anxiety, and ADHD.
By college I knew my ADHD diagnosis meant I wasn’t neurologically typical — it didn’t make me feel good, despite the diagnosis explaining stuff — removing a lot of self-blame and self-loathing I was feeling. Especially in grad school, when I started doing research, I learned how many things about me were ADHD, things that I had no idea were related.
Besides anxiety and depression, another thing I struggle with is working memory, never knowing where my keys are, having to walk across my apartment five times before I figured out what I’m doing. Getting that understanding from reading helps. It’s empowering to read about it and be able to connect to it and understand it—well, because I’m experiencing it.
At first, thinking of ADHD as a disability led to lower self-esteem. But, in terms of neurodiversity, stuff that had dragged me down felt more uplifting, especially over the last five years or so. I don’t have to feel lesser than other people and can recognize the things about ADHD that are advantages. It has been a big lift for my self-esteem.

One positive thing I can think of is creativity — this is big in ADHD people. It’s enhanced my art. Another is hyperfocus, which is when we’re in the zone. We get super focused on one task and become efficient and good workers. That’s special. I didn’t recognize it when I got in that kind of flow state. I thought that was how all people worked.
As a kid, videogames played into that hyperfocus, but they were also satisfying because of short-term reward loops — something highly rewarding and engaging for the ADHD brain. The only times that ever happened to me outside videogames was with art — getting to a flow state only happens when I’m making art. Even though I’m good at the technical skills I have, hyperfocus doesn’t happen. —Etan Swan
Musings on Female ADHD
Most ADHD research has focused on boys, so there’s less on how it differs in female biology, writes an Australian psychotherapist in Until Now Therapy. “Girls are extremely good at adapting and shifting to meet societal norms/expectations and therefore masking their difficulties…. They will heavily self-monitor their behaviors to get accepted and will adapt accordingly for the promise of social reward.”

Source: Susan Fishman, “7 Tips for Moms with Adult ADHD,” Healthgrades
Loudness becomes quiet but anxious. Impulsiveness becomes internal noise or online shopping. Being messy is obsessive cleaning and meticulous planning. Rage becomes depression. [Girls would do anything not to be] found out and be told “you don’t fit in here.” So, when environmental stress happens, the mask slips as the coping strategies go out of the window. This leads to further dysregulation (quick to anger, anxiety, depression responses) and a rapid drop in self-esteem. A female may present at the doctor and be faced with a list of inadequate diagnoses, often bipolar, anxiety, or even personality disorders—when maybe it’s ADHD. —Anonymous, “A Neurodivergence Journey – What lies beneath?,” Until Now Therapy
Coming Up Next
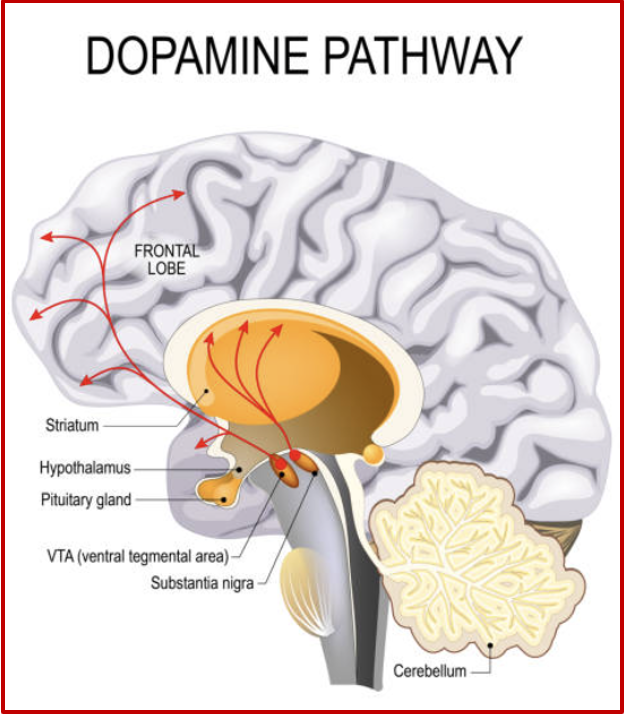
In Post 21: ADHD: A Preponderance of Risk Factors and Symptoms, I discuss dopamine deficits as a defining characteristic of ADHD and two opposing characteristics of ADHD not recognized in DSM-5: rejection sensitive dysphoria (RSD) and recognition responsive euphoria (RRE), one debilitating and the other exhilarating.
Copyright ©2026 Jan Swan