On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
23. ADHD: Named, Renamed, Still Needs a New Name

My sons, diagnosed with ADD as children, didn’t relate to being rediagnosed with ADHD as teenagers, because they weren’t hyperactive (H). Now, as adults they don’t appreciate the words deficit (D) and disorder (D). That leaves attention (A). You can find the same discontented voices on social media. A great many people also don’t like hyperactivity since their symptoms are not a match. Even though DSM-5 allows for that in its subtype — ADHD: predominantly inattentive — no one reads DSM-5. People go through their lives stigmatized at school or work, in the playground, in the doctor’s office.
Photo: iStock
ADHD and Reward Deficiency Syndrome
It’s more than pickiness — it’s about being tired of forever second-class status. Never doing it quite right. Too many mistakes, not fast enough or too fast, never completed or if completed never handed in. A little bit more crushed by each critical comment or unfriendly face. So, they turn inward to distract from the shame, or they stop trying. Yet the reality is wholly different.
My sons have so many extraordinary qualities, artistic skills, and unusual outlooks on life. They’re such caring people. They have no problem with “hyperfocus” when they’re highly engaged in what they’re doing. They like videogames because they’re energized by that hyperfocus. People with ADHD can be resilient, creative thinkers, big picture people, spontaneous, with energy for new experiences. Not all the qualities at the same time in the same person—but if not trodden down by the unrelenting stress of trying to succeed in a neurotypical world, they would benefit society in so many ways. It’s for these reasons that ADHD has to go as a moniker for this neurological condition. As the next section will show, naming this condition has a long history.
From Clumsy Child Syndrome to ADHD
Originally called hyperkinetic reaction of childhood or minimal brain dysfunction, British pediatrician Sir George Frederic Still described it in 1902 as “an abnormal defect of moral control in children.” He wrote about intelligent children exhibiting inattentiveness, impulsivity, and hyperactivity. At other times, doctors and scientists used the terms clumsy child syndrome and organic brain disease.
In 1939, the U.S. Food and Drug Administration (FDA) approved Benzedrine (a narcotic amphetamine) as a medication. Psychiatrist Charles Bradley “stumbled across some unexpected side effects of this medication … young patients’ behavior and performance in school improved when he gave it to them.” Years passed before researchers recognized the benefits of Bradley’s discovery.
In 1955, FDA-approved Ritalin (psychostimulant methylphenidate) superseded Benzedrine as the medication of choice once the disorder was better understood and diagnoses increased.
In 1968, APA’s 2nd edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-2) recognized hyperkinetic reaction of childhood.
Photos: Sir George Frederic Still and Charles Bradley, Wikipedia

A Changing Definition
In 1980, DSM-3 published the renamed attention deficit disorder (ADD) with two variations: ADD with hyperactivity and ADD without hyperactivity.
In the 1987 revised DSM-3, the name changed to attention-deficit/hyperactivity disorder (ADHD), reflecting all three characteristics of inattention, hyperactivity, and impulsivity—without requiring the presence of all symptoms to be diagnosed.
No further changes came until 2000 when DSM-4 included three ADHD types still used today: combined, predominantly inattentive, and predominantly hyperactive-impulsive types.
Source: Laura Porter, Very Well Health
The ADHD Community Speaks Out
Since 2000, the medical/psychiatric and governmental/ insurance complex has fully absorbed and accepted ADHD for purposes of diagnosis/treatment/legal protection/health coverage. As a term it seemed acceptable. Attention-Deficit/Hyperactivity Disorder.
But during these intervening 25 years, the neurodiversity movement happened—and with it raised consciousness about calling neurodivergence a “deficit disorder” or any other pejorative characterization.
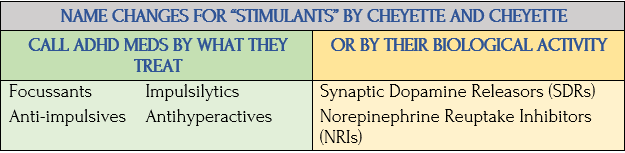
In their Psychology Today article, “Why ADHD Should Be Renamed,” Benjamin Cheyette and Sarah Cheyette make the case for a name change, as charted here [paraphrased/edited]:
Source: Laura Porter, Very Well Health

Source: Benjamin Cheyette, psychiatrist/professor emeritus, UC San Francisco, and Sarah Cheyette, pediatric neurologist/author, Winning with ADHD
Combined Type ADHD
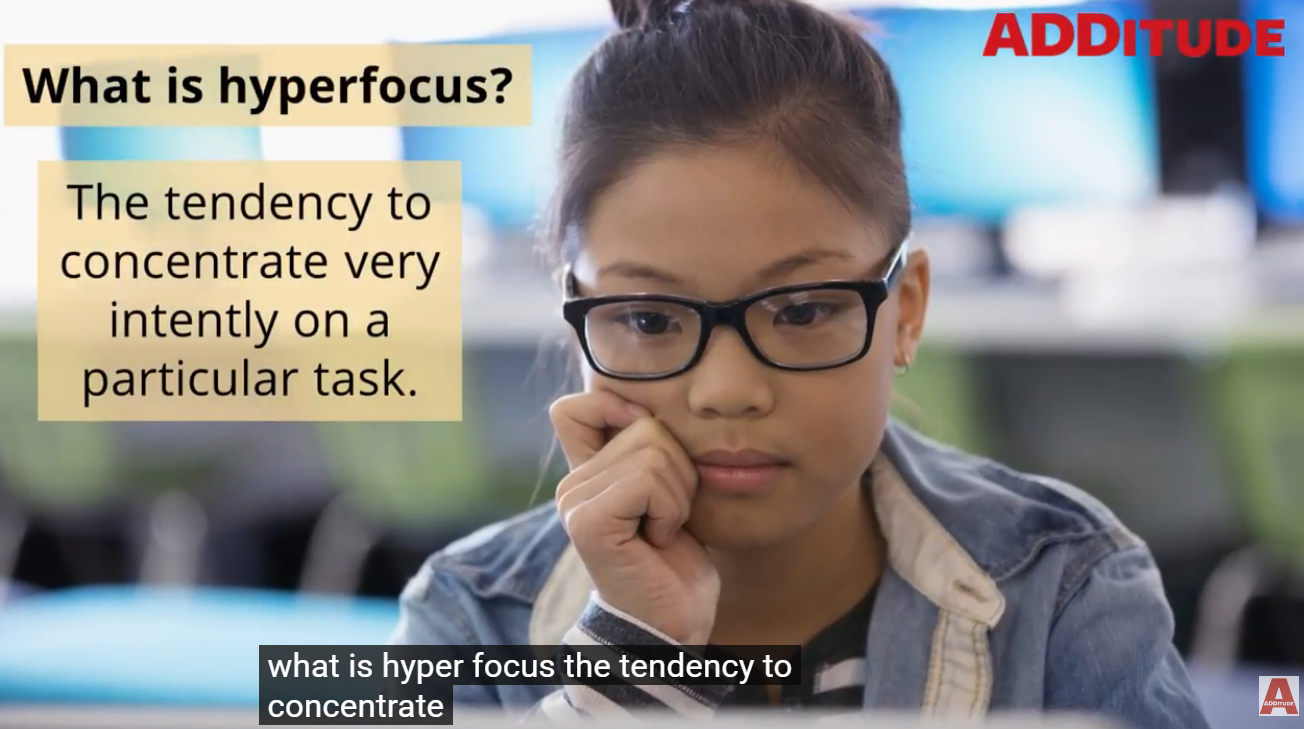
Hyperfocus is a common, but confusing symptom of ADHD. How can someone be distractible, but also have a hyper fixation on an interesting task? Royce Flippin, “What Is ADHD Hyperfocus?, ADDitude videos
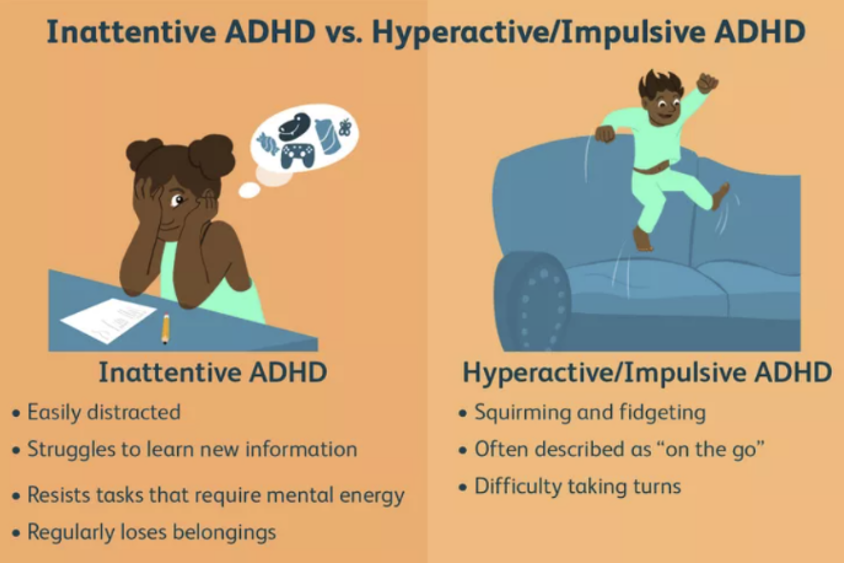
The Cheyettes discuss the contradictions in ADHD’s two major behavioral domains. First, attention deficit suggests ADHD’ers can’t pay attention when they can. Sometimes they pay attention to trivial, time-consuming things that might even indicate maladaptive behavior, often called hyperfocus. But this is not a deficit. They write, “It’s more accurate as a difference in the balance or regulation between two natural states of mind.” Second, hyperactivity, when juxtaposed against attention deficit, creates more confusion. Many with inattention don’t have hyperactivity/impulsivity, and ditto in reverse. Some with hyperactivity/impulsivity don’t have problems with inattention.
The term disorder is also controversial. Although negative features are what get treated, there are positive aspects to ADHD. When the ADHD brain doesn’t focus where it should (classroom teacher, work project), a different natural brain activity engages — looking at the “big picture” over details (forest vs trees).
Or the ADHD brain may be in “search mode” — scanning for something more salient or important compared to the task everybody around them is focused on. This is not necessarily a bad trait. There are situations that could benefit the ADHD person and their societal group (family, clan, tribe, or country).

Source: Keith Low, “ADHD in Children: Symptoms and Treatment,” Very Well Mind
ADHDers can be movers and shakers, learn early in life to appreciate their independence, and be more comfortable with change — less committed to the status quo. They tend not to respond well to delayed gratification, but the reverse of that is they’re oriented toward immediate results. The Cheyettes write, “Their energy and daring combined with ability to initiate new directions can be a recipe for success.”
In their Scientific American article, “We Need to Rename ADHD,” Branko van Hulst, et al., note the potential outcome of labeling children. I paraphrase:
A child is called inattentive at school. At this point, the only known is the child is inattentive because of their inattentiveness. If we say the child has an attention deficit, we are inclined to look for the cause of the problem. But when we say the child has an attention deficit disorder, we might assume we know the cause: they have a disorder or, at least, they have an issue in their brain. The reason this is more than an innocent mistake is because a “disorder” systematically places the problem with the individual, diverting focus away from the context (family/school/work) where traits lead to problems.
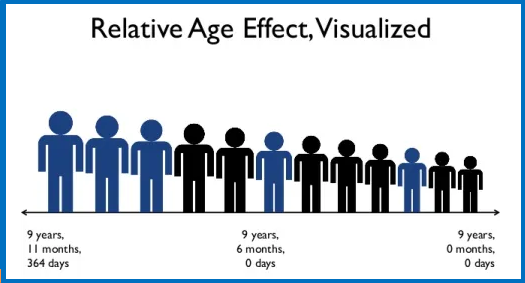
ADHD and Relative Age Effect
One of the clearest demonstrations of context shaping diagnosis is the relative age effect.
The following includes findings from research by Branko van Hulst, child/adolescent psychiatry resident, Leiden University Medical Center (LUMC), Sander Werkhoven, assistant professor, Ethics Institute, Utrecht University, and Sarah Durston, professor of development brain disorders, University Medical Center Utrecht (UMCU). Their article is based on research sponsored by Dynamics of Youth of Utrecht University:
- A compelling example of relative age effect is how the youngest students in a class get diagnosed with ADHD more often and receive more ADHD medication than their older classmates. Relative immaturity can be mistaken for ADHD — a consequence of these children being unfairly and unfavorably compared to their older classmates
“Relative Age Effect in Irish youth football,” Talent Development in Irish Football
- It’s a mirror image of the well-known relative age effect in professional sports, where relative maturity in young athletes is mistaken for talent.
- Since the term ADHD implicitly refers to a known cause, it provides a distinct explanation and a clear perspective for treatment. The question “How can we best handle this child’s difficulties in this particular context?” is replaced by “How can we best treat their ADHD?” Perhaps this child is given medication, when instead delayed school entry might have fit their developmental profile.

Graphic: Russell Barkley, Wow Occupational Therapy
- Other societal elements affecting a child’s individual context but perhaps getting overlooked (divorce, sleeping problem, poverty) can lead to overall lower rates of ADHD. The authors write, “We would like to argue that the biggest risk lies here: by presenting psychiatric classifications — ADHD in this case — as explanations rather than descriptions, we risk overlooking a variety of societal options to increase children’s wellbeing.”
According to clinical neuropsychologist Russell Barkley, ADHD children are typically 30% behind their peers with executive functioning skills. He coined the term “executive age” to illustrate how mental processes involved in problem-solving, goal-setting and planning, and managing (time, emotions) are behind developmentally. This diagram shouldn’t be taken literally for the numbers, but for the idea behind delays.
In sum: These findings don’t mean ADHD is not a genuine neurodevelopmental disorder. Rather, they suggest that for some children — particularly those near the diagnostic threshold — the educational context and timing of school entry may influence whether typical developmental variation is viewed as evidence of disorder. What’s good to know here is that a diagnosis should describe clinically significant patterns of difficulty, along with careful consideration of developmental stage and the child’s broader social and educational context.
Is ADHD a Spectrum Disorder?
A spectrum contains everything. Source: MicroOne/Shutterstock
In their PubMed Central/NIH paper, “Changes in the Definition of ADHD in DSM-5: Subtle but Important,” Jeffery Epstein and Richard Loren, raise issues not addressed in ADHD revisions in DSM-5. I paraphrase and edit for brevity:
- There’s increasing, but not universal, acceptance that ADHD is a dimensional disorder. Inattention and hyperactivity/impulsivity are behavioral traits that naturally occur on a continuum, like intelligence.
- Diagnostic thresholds that define “abnormal behavior” are artificial, though useful in identifying individuals who experience significant impairment in daily functioning.
- While DSM-5 classifies severity (mild, moderate, or severe), these can be applied to specific symptoms or to the magnitude of impairment. But this is unreliable and varies considerably.
Epstein and Loren don’t comment on whether ADHD should be reclassified as a spectrum disorder. But the Cheyettes offer strong words of caution, writing the practice of referring to behavioral conditions as “spectrum disorders” shouldn’t become accepted diagnostic practice. The problem is that ALL human behavior exists on a spectrum. They write, “Nearly everybody has gone through experiences, circumstances, or times when they were a little depressed, a little anxious, moody, irritable, overly-confident, self-inflated, shy, socially awkward, inattentive, or impulsive.”
DSM-5 states there must be “clear evidence the symptoms interfere with, or reduce the quality of, social, school, or work functioning.” The Cheyettes write, “We support continuing the use of severity criteria to justify psychiatric diagnosis. Although all human behavior exists along a spectrum, a line has to be drawn somewhere between normal variation vs medical conditions that warrant a diagnosis, treatment, and accommodation by the rest of society. ‘Spectrum disorders’ should not become the norm for psychiatric diagnostic practice.”
Citation: Jeffery Epstein and Richard Loren, Behavioral Medicine/Clinical Psychology, University of Cincinnati College of Medicine, and Cincinnati Children’s Hospital Medical Center.
What To Call ADHD
What To Call ADHD
The Cheyette team counsels finding a solution to renaming ADHD is to focus on “psychiatric conditions according to their biological basis …. In the future, many psychiatric diagnoses, not just ADHD, are likely to be reified, re-aligned, and relabeled according to a more solid scientific understanding of their underlying biological causation.” So they suggest:
Dopamine Transporter Deficiency Amygdala-BNST Circuit Sensitivity Left Fronto-Cortical Hypoactivity
Since none of those are likely (amygdala-BNST circuit, really?), they do come up with a menu of alternatives.
Cheyette Team’s Menu of ADHD Name Replacements
Must use some combination of the following terms: attention, focus, impulse activity, movement, energy regulation/ dysregulation, balance/imbalance:
Attention, Impulse, or Activity Dysregulation / Focus, Impulse, or Movement Regulation Imbalance
Attention/Focus, Impulsive, Energy Regulation (AFIRE) / Impulse Movement and Energy Regulation
An Argument for VAST: Variable Attention Stimulus Trait
Writing in ADDitudemag, world-renowned ADHD experts/physicians Edward Hallowell and John Ratey declare, “ADHD needs a better name, and we have one.” Better than ADHD?
ADHD is an inaccurate — and potentially corrosive — name. The term “deficit disorder” places ADHD in the realm of pathology, or disease. Individuals with ADHD do not have a disease, nor do they have a deficit of attention; in fact, what they have is an abundance of attention. The challenge is controlling it.
Therefore, we argue that a more accurate descriptive term is variable attention stimulus trait (VAST), a name that allows us to “de-medicalize” ADHD and focus instead on the huge benefits of having an ADHD brain.
VAST symptoms can, of course, negatively impact a person’s life, work, and relationships. Rejection sensitive dysphoria (RSD), a phrase coined by Dr. William Dodson, refers to the extreme emotional sensitivity and feelings of guilt, shame, and rejection often experienced by those living with VAST.
But with VAST there are always pairs; you can hyperfocus and then you can’t focus. You are distractible, but you’re also curious. So if individuals with VAST tend to succumb to perceived rejection, they can just as easily thrive with perceived recognition, an experience we call recognition responsive euphoria (RRE). —Physicians Edward Hallowell and John Ratey, ADDitudemag
[See post 21 for a description of Dodson’s RSD and Hallowell and Ratey’s RRE]
Meet ADH: Attention-deficit (and/or) hyperactivity. No surname.
Before I list reader recommended name changes, one more suggestion from experts from Utrecht University and Medical Center, Utrecht, Netherlands:
Our modification is as simple as it is effective: drop the term disorder from all classifications. Just drop it. In the case of ADHD, call it attention-deficit (and/or) hyperactivity. Nothing is lost in terms of definition, ease of communication, or accessibility to research; nor does it detract from the significance of the problems that people face. The only thing we would lose is the false suggestion that when we use a psychiatric name we understand the causes of the problem at hand. In its place, we would gain an incentive to see a child in his full context and explore all options for improvement. —”We Need to Rename ADHD,” in Scientific American, by Branko van Hulst, Sander Werkhoven, and Sarah Durston
Stop Calling ADHD Meds “Stimulants” vs “Non-Stimulants”
The Cheyettes also make a case for changing what we call ADHD meds. The term “stimulants,” which are pretty much only used to treat ADHD, causes a lot of misconceptions.
Paraphrasing the Cheyettes, who note: The name “stimulant” arose because they can make people feel more awake, but stimulation isn’t the therapeutic goal for treating ADHD — it’s a side effect. “It’s unprecedented in medicine to call a medication by its side-effect profile. That’s like calling antidepressants and antipsychotics ‘appetite inducers’ or ‘hypometabolics,’ because they often make people gain weight. Non-stimulant is even worse: calling a medication by what it is not! There are literally no other medications we can think of that are named by such a convention.”
ADHD Name Change Ideas
Image: Tik Tok
Many want to see a name change that elevates ADHD’s strengths and advantages, not just its challenges. ADDitude asked its readers whether they thought ADHD was a terrible name for the condition: 52% said yes, 34% were neutral, and 14% were ok. Here are ADDitude readers’ suggestions for an ADHD name change:
Neuro Spicy / Zoomies / Racecar Brain
Capacity Management Syndrome (CMS) / Neuro-Overload Disorder (NOD)
Exceptional Artistic Ability of the Genius Variety
Can’t Live Up to Your Bullsh*t Expectations Syndrome
Variable Attention Trait Disorder (VAT)
Executive Malfunction Disorder / Emotional Regulation Disorder
Dysregulated Attention Disorder (DAD) / Selective Attention Impulsive Disorder (SAID)
Chronic Overwhelm Disorder (COD) / Dopamine Attention Variability Executive Dysfunction (DAVE)
Jan Swan’s Re-Name for ADHD
I can’t help but toss my hat into the ring: Attention NeuroDivergence (AND)
I know, it’s confusing when you write “… and AND” but otherwise, it’s pure genius. Since no one will know what I’m talking about if I use AND, I will resign myself to calling it ADHD. Sometimes Zoomies can’t swim against the tide.
Coming Up Next

In Post 24: ADHD: Treatment and Coping Skills for All Ages, I discuss ADHD symptoms, treatment, and coping skills.
Sources
Copyright ©2026 Jan Swan