On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
22. ADHD: Inattentive, Impulsive…and Hyperactive?
Hyperactivity decreases with age, but most people with ADHD don’t grow out of childhood difficulties with restlessness, focus, or impulsiveness. Behavioral symptoms can be so “pervasive and persistent” that every aspect of life is affected. Problems at school become problems at work — both finding it and keeping it — while living in fear that you don’t meet expectations, that you will be excluded or confronted. You wear your normal mask even when over-stimulated by a fragmented, noisy world not of your choosing. ADHD affects relationships, vulnerabilities, and self-regard — and an ability to harness your creative energy without burning through the goodwill of those who get close. ADHD is a hallmark of the neurodivergent mind.
Graphic: ADHD Inattentive VS Hyperactive Kids, Goally
Essential to any ADHD diagnosis are:
ADHD and Reward Deficiency Syndrome
- Poor attention/persistence, particularly if tasks are boring, tedious, take too long, or repeat, often losing/interrupting concentration due to irrelevant thoughts or external events — heightening distraction.
- Poor impulse control/delayed gratification, not thinking before acting, working for larger, longer-term rewards.
- Excessive, unfocused, unregulated activity, struggling to control activity level, engaging in inappropriate behaviors.
Graphic: Timothy Wilens, et al., “Presenting ADHD Symptoms, Subtypes, and Comorbid Disorders in Clinically Referred Adults with ADHD,” The Journal of Clinical Psychiatry, PubMed
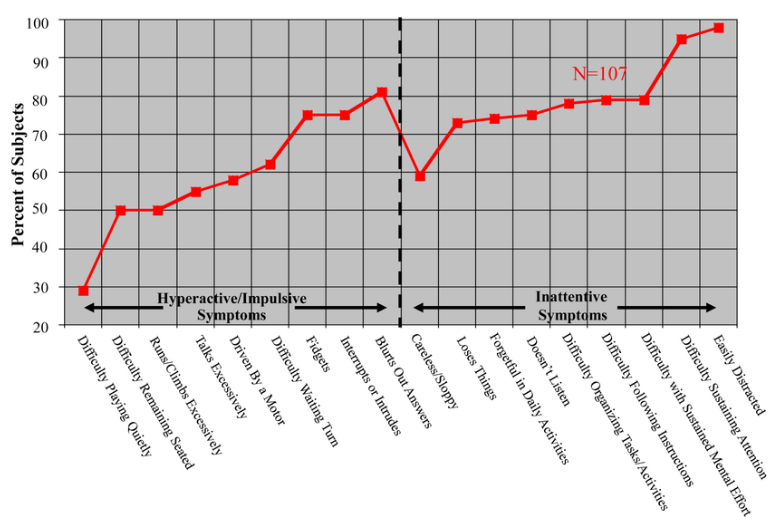
Research Breakthroughs
After thousands of studies over the past century, a recent research breakthrough found people with ADHD don’t have the same traits. Ever since, ADHD continues to get updated with new research.
In their PubMed Central/NIH study of ADHD adults, Timothy Wilens and colleagues found an overwhelming 93% of participants have prominent symptoms of inattention — based on DSM-5 criteria defining both predominately inattentive and combined types.
This and other studies support findings of impaired neuropsychological functioning, working memory (short-term/temporary memory essential to complete cognitive tasks), and cognitive control (executive functioning) in ADHD adults.
The Wilens study also found that adults with combined-type ADHD had higher rates of psychiatric comorbidity — including autism, bipolar disorder (BD), psychosis, conduct disorder (CD), and personality disorders (PDs) such as borderline personality disorder (BPD) — than adults with predominantly inattentive ADHD. These findings have important implications for both diagnosis and treatment.
In addition:
- It remains difficult to determine whether greater ADHD symptom severity contributes to psychiatric comorbidity, or whether comorbid conditions inflate ADHD symptom counts.
- Although adults with inattentive ADHD had lower rates of several disorders than those with combined type, they still experienced substantial psychiatric and substance use comorbidity that may be missed because their symptoms are less outwardly disruptive.
- Psychiatric comorbidity was associated with more persistent and severe ADHD, particularly prominent hyperactive-impulsive symptoms.
- Adults with combined type had significantly higher rates of conduct disorder, bipolar disorder, and psychosis than those with inattentive type. This parallels other research showing that adult hyperactive-impulsive symptoms are more strongly associated with BPD than are predominantly inattentive symptoms.
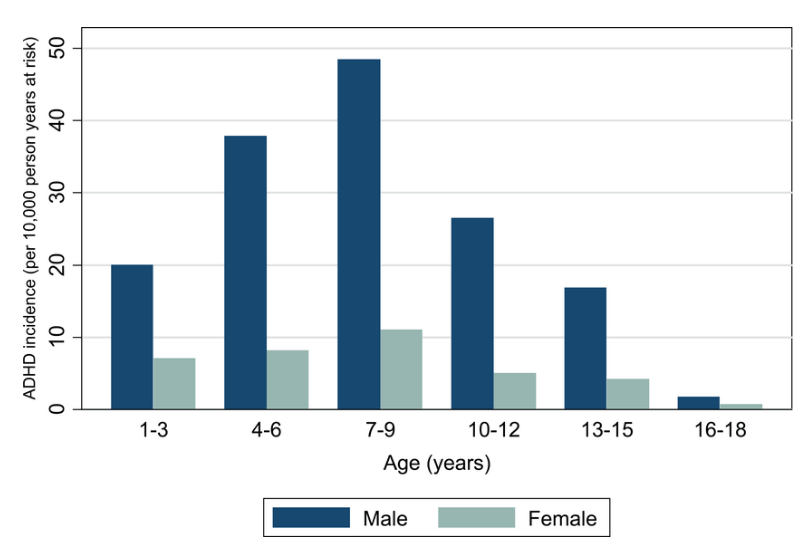
ADHD incidence by age of diagnosis. Adrian Hire, et al., “ADHD in the United Kingdom: Variations in Incidence Rates Among Children and Adolescents,” ResearchGate
This study had equal men/women and found no sex differences in symptoms. Men/women had equivalently high rates of inattention relative to hyperactivity/impulsivity. Difference does show up in comorbidity:
- ADHD males had higher lifetime comorbidity with conduct disorder and alcohol abuse.
- ADHD females had higher rates of comorbid dysthymia (persistent, mild depression), panic disorder, agoraphobia, specific phobia, and generalized anxiety disorder (GAD).
Natural Ways to Increase Dopamine Levels
Since dysfunction in the brain reward cascade can lead to low dopamine levels, the brain requires more dopamine to avoid feeling uncomfortable. Stimulants target dopamine, but natural ways can boost it as well.
- Consistent, relaxing sleep routine
- Quick activities, like jumping jacks, coffee, or listening to a favorite song
- Several mini-meals throughout the day
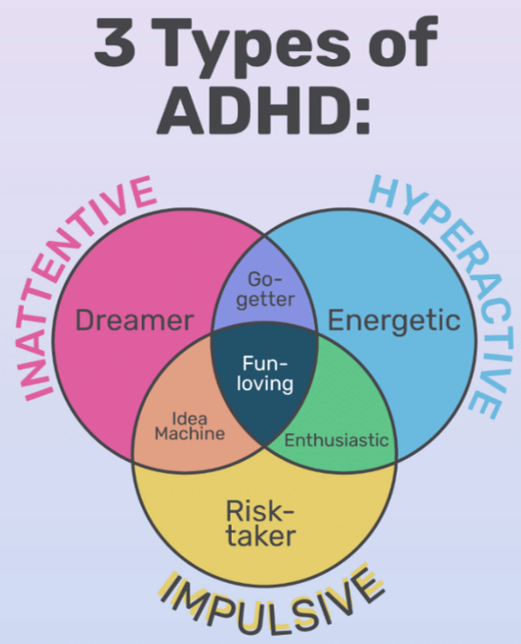
Three Main ADHD Types
Graphic: Very Well Mind
Combined Type ADHD
Around 70% of ADHD clinical cases are diagnosed as combined type within 3-5 years of initial diagnosis, with all five symptoms:
- Early onset of symptoms. 50% of cases start by ages 4-7 and nearly all cases by 14-16.
- Impaired cognitive control (executive function/EF) — ADHD’s most debilitating feature, affecting motivation and working memory. This leads to poor self-control, muddled thinking, and not seeing future consequences of current actions. Research suggests childhood EF predicts academic/work functioning, regardless of intelligence or social class. A cohort study of 1,000 children, birth-age 32, showed EF predicted physical health, substance dependence, personal finances, and criminality.
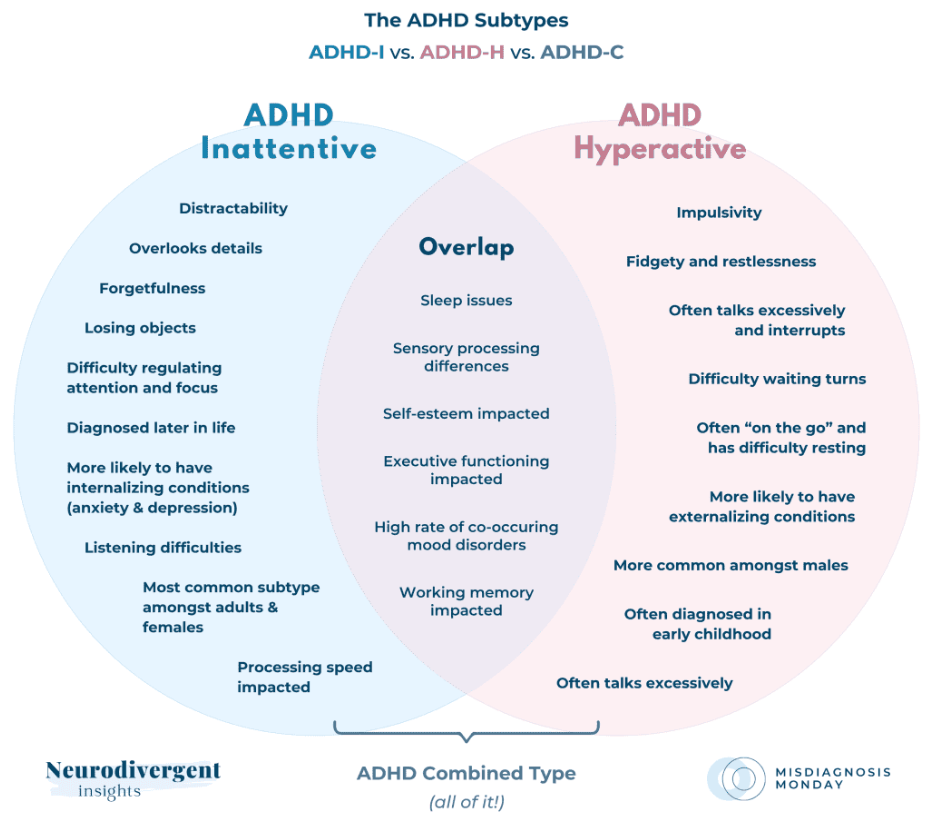
Graphic: Megan Anna Neff, Neurodivergent Insights

Graphic: Megan Anna Neff, Neurodivergent Insights
- Highly variable, inconsistent performance of tasks over time. In school/work activities, ADHD’ers are better one-on-one over group and new, engaging over repetitive, familiar. They focus more on completing tasks for authority figures or if there are consequences.
- Trouble following directions, instructions, rules is harder for ADHD’ers, particularly without supervision — which has nothing to do with comprehension, defiance, or memory impairment.
- Relatively chronic course. Most with ADHD lag behind their age group in sustaining attention, inhibiting behavior, and controlling activity levels.
Predominantly Inattentive Type ADHD

Photo: Christine Merrell, “Inattentive behavior in the classroom, Cambridge University Press
Recognized in 1980, this type represents 14%-20% of all clinical cases, with some experts believing it’s a milder form of combined type. Attention and organizational problems require mental effort due to being easily distracted, making careless mistakes, not listening well, or losing/forgetting. But they don’t have excessive activity levels or poor impulse control. There are two main subtypes:
Sluggish Cognitive Tempo (SCT): Up to half of attentive type cases have SCT, a more excessive version — with some arguing it may be a separate disorder:
- Hypoactive, daydreaming, slow, easily confused, lethargic, mentally “foggy.” Not too responsive to stimulants.
- Poor, selective attention. Error-prone information processing—hard to prioritize what’s important. More erratic retrieval from long-term memory.
- Impaired school performance, learning disabilities are 20%-50%, with more dyscalculia (math understanding)
Socially reticent, shy, withdrawn. Not impulsive or aggressive. Responds well to social skills training. Greater risk of anxiety and depression.
Predominantly Hyperactive-Impulsive Type ADHD

Recognized in 1994, predominantly hyperactive type ADHD shows impulsive, hyperactive behavior in 7%-15% of cases. May be a developmental stage of combined type.
Hyperactivity: Younger children don’t stop running, climbing, fidgeting, squirming. Older children, teens, and adults might be extremely restless, unable to wait, take turns, engage in activities quietly. Wear others out with constant activity.
Impulsivity: ADHDers of any age can act impulsively, talk excessively and inappropriately, interrupt others, or listen to directions. Younger children may grab things from others. Older children may have more accidents and injuries than others.
Motor Planning and Motor Timing in ADHD
In addition to cognitive/behavioral challenges, many children with ADHD have motor planning and timing issues, both involving motor cortex activity in the brain. These functions are distinct but interconnected. Effective motor planning facilitates motor timing by creating well-structured though adaptable movement plans.
Motor Planning

Photo: Offset, Shutterstock
According to North Shore Pediatric Therapy, children with motor planning difficulties don’t learn as easily from trial-and-error feedback, even with familiar tasks. They can appear clumsy, slow to learn basic skills, and take longer than other children to put on a jacket or ride a bike.
Motor planning deficits affect how children do in school, since physical tasks can be difficult. These issues may be partly problems with movement and coordination — a common symptom in developmental coordination disorder (dyspraxia), as well as in ADHD. Other ADHD motor problems include difficulty with handwriting and other muscle, movement and balance problems.
Variable Motor Timing (VMT)

Another brain function adjusts movement speed/rhythm. VMT is the flexible, dynamic adjustment of movement timing necessary to complete a planned motor action. Baseball players adjust their bat-swinging timing based on anticipated speed or curve of the pitch. We constantly rely on real-time sensory feedback to adjust. Motor timing is either explicit (managing time to meet a deadline) or implicit (rhythm of daily routine or interpreting an event).
Poor variable motor timing is core to ADHD, characterized by slower/more variable reactions and decreased/inconsistent accuracy. Studies show stimulant medication, the most effective treatment for ADHD, can reduce/normalize impaired VMT.
Spontaneous Motor Tempo (SMT) and Other Timing Issues

Photo: Shutterstock
Turns out we each have a preferred tempo for movement — our easiest, most natural pace to move. SMT is roughly two movements/second for adults, slightly faster in children, and slower in the elderly. ADHD shows deficits in SMT and other timing functions: perceptual timing (estimating time intervals) and temporal foresight (considering future consequences of behavior). [Sources: North Shore Pediatric Therapy, Wikipedia, and research by Anat Dahan and Miriam Reiner, “Evidence for deficient motor planning in ADHD,” Scientific Reports, Nature]
ADHD and Social Issues

We need more research on ADHD and social impairment. ADHD is a condition of executive function (EF) impairment, and social cognition is a part of that. Impulsivity and inattention, as well as symptoms from comorbid issues like oppositional behavior or anxiety, can lead to awkward, uneasy socializing.
Research finds people with ADHD may have:
Photo: Adobe Stock
- Social knowledge deficits: A lack of basic understanding of social rules, norms, and expectations leads to difficulties in navigating social situations.
- Neuropsychological impairment: In addition to cognitive/EF deficits, there can be difficulty with social and/or emotional distress.
- Social information processing deficits: Cognitive processing impairment can lead to inaccurately perceiving, interpreting, and responding to social cues — like misreading facial expressions, body language, tone of voice, or perceiving hostile intentions where they don’t exist — often resulting in inappropriate or maladaptive behaviors.
Social problems have been reported in 52%–82% of children with ADHD and are increasingly seen as an important associated feature of the disorder. Impairment in social functioning has been reported by parents, teachers, and peers — and documented as early as the preschool years.
Children with ADHD are rated lower on social preference (making decisions, people-pleasing behaviors), have fewer reciprocated friendships, and are more often disliked by their peers, as soon as the first day or even within 20 minutes of the social interaction.
Peer rejection … has been associated with negative long-term outcomes, including substance abuse, school dropout, delinquency, academic problems, and higher rates of psychopathology. Further, rejection limits a child’s opportunity to practice social skills and as such exacerbates social problems. Importantly, social difficulties are not limited to childhood and account for frequent job loss and increased divorce rates in adults with ADHD. —Ekaterina Sotnikova, et al., “Pragmatic Deficits and Social Impairment in Children with ADHD,” PubMed Central/NIH
Of course, not everyone with ADHD has all these symptoms. Ekaterina Sotnikova, et al., PubMed Central/NIH, writes “support for these explanations have been inconsistent” and “existing treatments for ADHD, though helpful in treating core symptoms, have limited effectiveness at improving social skills.” She says social deficits are not fully explained by ADHD, and lacking social knowledge is not the reason for the amount of social impairment that some with ADHD have.
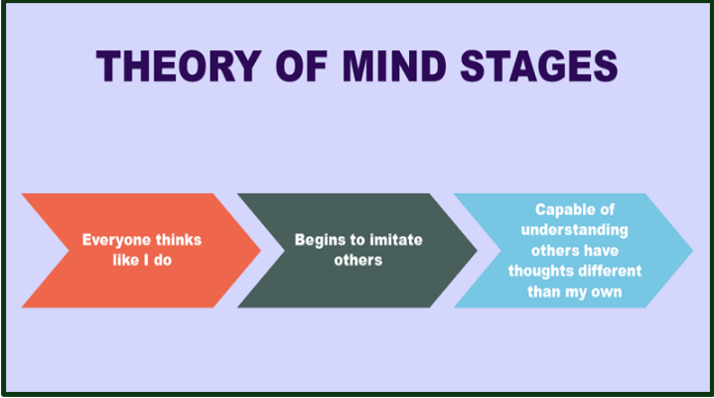
Theory of Mind (or Social Cognition)
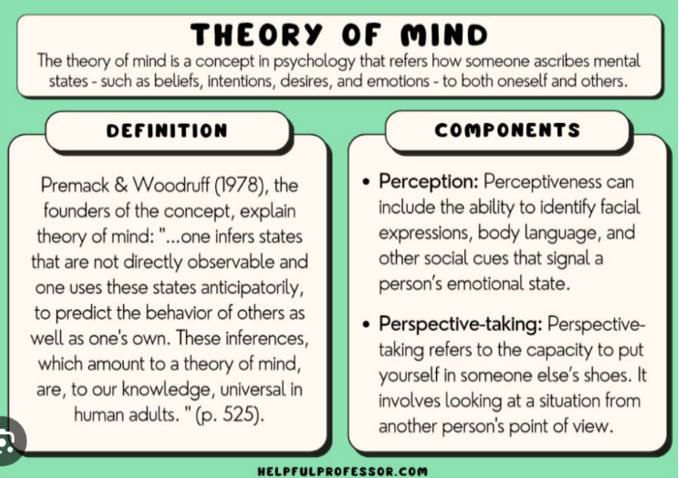
Written by social work educator Gregory Paul C. (MA), Helpful Professor
Theory of Mind (ToM) is key to successful social interaction. It’s what we think of other people’s “mental states” — beliefs, desires, emotions, thoughts — and how they differ from us. And why. ToM’s are not predictions of what’s about to happen — what we can’t know — but theories based on what we understand about them and what we can infer about their intentions.
In ADHD, impaired EF leads to impaired ToM, especially working memory, planning, and inhibition. A person’s social interactions can be affected by misinterpreted social cues, inappropriate comments, seemingly little empathy [see post 36] — and generally finding it difficult to make friends.
Studies show children and adults with ADHD often perform lower on ToM tasks compared to neurotypical individuals, especially when assessing complex emotions or subtle social cues.
ADHD Prevalence
ADHD diagnoses have been on the upswing for years now, in all countries and ethnic groups that have been studied to date. Here’s some hard data about its prevalence.
ADHD Prevalence by Demographics
- Overall prevalence of ADHD children (ages 3-18) increased by 42% from 2003 (8%) to 2011 (11%) — a total of 6 million children.
- Further breakdown: ages 3-5: 265,000 (2%), with age 6 most common for onset. Ages 6-12: 2.4 million (10%); ages 13-18: 3.3 million (9%-13%)
- Another survey gives a broader range of 2%-18% of all school-aged children and adolescents, and 5% of ADHD adults.
- Boys (13%) are 3 times more likely to be diagnosed than girls (4%-6%), but girls are likely underdiagnosed due to differences in symptoms and an unequal focus on males in research.
- Black, White, and non-Hispanic children are more often diagnosed (10%-12%) than Hispanic (8%) or Asian (3%) children.
ADHD Prevalence by Impairment
- A survey of teens showed 9% with ADHD, nearly half (4%) with severe impairment.
- Nearly ½ of ADHD children have severe impairment into teens, due to comorbid mental, behavioral, and neurodevelopmental disorders, lower intellectual and/or social functioning.
- 75% of U.S. children experience symptoms as adults, with 15%-14% outgrowing their symptoms. Recent studies suggest 66% are significantly impaired by symptoms as adults.
- An international survey showed symptoms remain stable through adolescence, with 1/3 of ADHD children experiencing impairment as adults.
- Hyperactivity is less overt with age, but still have inattention, impulsivity, and restlessness.
- Females: more likely to have inattentiveness. Males: hyperactivity and impulsivity.
ADHD Causes
ADHD diagnoses have been on the upswing for years now, in all countries and ethnic groups that have been studied to date. Here’s some hard data about its prevalence.
ADHD Risk Factors

Photo: Getty Images. Credit Shutter2U
Genetic: There’s no single cause for ADHD. Yet evidence supports its genetic basis — accounting for 65%-75% of all cases. ADHD:
- Occurs far more in biological families, especially identical twins. May be associated with gene variations regulating the brain’s dopamine activity.
- Likely arises from a combination of risk genes. Genetic testing may lead to accurate diagnosis, with targeted medications for different genetic subtypes
Brain injury: 35% of ADHD cases stem from brain injury or disrupted brain development:
- Include: smoking in pregnancy, pregnancy/birth complications, maternal alcohol use, lead poisoning, bad reactions to bacterial infections, or head trauma, brain tumors, or stroke.
- Individuals with seizures or epilepsy are 2-3 times more likely to have ADHD.
- Sedatives or anticonvulsant drugs can lead to ADHD or make pre-existing ADHD worse.
Not a cause: Research doesn’t support ADHD being caused by consuming food additives, preservatives, or sugar — though allergies can worsen symptoms.
ADHD Risk Factors

Photo: Getty Images/iStockphoto
Anyone with ADHD can be successful in school/worklife, but it takes lots of treatment and support. Without treatment, consequences tend to be much more severe.
School failure: Impaired EF can lead to poor academic performance/achievement — and result in learning disabilities.
Delinquency, aggression, conduct problems: Studies suggest 45%-84% of those with ADHD have anti-social behavior or show verbal/physical aggression — as in oppositional defiant disorder (ODD) or conduct disorder (CD) — being defiant to adults/authorities, stubborn, disobedient, or destructive.

Photo: Jose Luis Pelaez Inc/Digital Vision/Getty Images
Excessive emotional displays/immaturity: Children may show exaggerated emotions due to lower frustration tolerance or greater emotional sensitivity. Low self-esteem is common by “tweens.” Individuals of any age are at risk for anxiety, depression, other mood disorders.
Social relationship problems: One half of those with ADHD struggle with social relationships or resolving conflicts with family members, peers, others — causing stress and disruption.
Other challenges associated with ADHD: Accidental injuries, substance abuse, job failure.
Traditional Evaluation and Diagnosis

For a diagnosis, behavioral/psychological, educational (if relevant), and medical specialists conduct a comprehensive assessment to identify underlying neurocognitive deficits. ADHD symptoms can include EF and motor deficits, as well as delay aversion and poor conflict detection [see post 20].
The World Health Organization (WHO) defines ADHD as requiring inattention, hyperactivity, and impulsivity symptoms to be present [all ages], especially starting early childhood. Symptoms must be “persistent across time, pervasive across situations, significantly out of keeping with developmental level, and have a direct negative impact on academic, occupational, or social functioning.”

Diagnosis in the US requires at least six symptoms in a child before age 12 and five in older teens/adults. Despite increases in adults, many psychologists don’t diagnose adult ADHD due to uncertain data on what it looks like. Also, adult ADHD has higher comorbidities that can lead to more severe/persistent symptoms. With irrefutable evidence that most people with ADHD have prominent inattentive symptoms, it’s even more important to look for this in the assessment.
Photo: PeopleImages.com
The “Transdiagnostic” Revolution

Image: Shutterstock
Worth mentioning is a nascent but growing use of a cross-diagnostic approach to assessing neurodevelopmental/mental disorders — cutting across traditional diagnostic boundaries found in DSM-5. My son with bipolar disorder, onset age 25, was diagnosed with ADHD in fourth grade. Treatment is not the same and can do harm [see post 14 on bipolar disorder]. Data on BD-ADHD correlation:
- Comorbidity and missed diagnoses: A 2021 meta-study found 1/3 adults with ADHD also had BD. 1/6 adults with BD had ADHD. With comorbidities, diagnoses are often missed. It can take up to 17 years for people to receive an accurate BD diagnosis.
- Genetics and risk factors: Relatives of people with BD are more likely to have ADHD, and vice versa. Up to 33 genetic risk loci (locations on the genome) are involved in both conditions. Maternal substance abuse and stress during pregnancy increases risk.
- Diagnosis: ADHD is often diagnosed first because symptoms usually appear in childhood, while BD is usually diagnosed in adulthood.
- Emotional dysregulation in BD-ADHD can be mistaken for hypomania.
While I have organized this blog around specific diagnostic conditions because that’s how the literature and available resources are organized, in practice individuals receive better, more effective care by the mental healthcare community taking this more holistic, do-no-harm approach. People need to advocate for themselves in accurately describing all symptoms and not just assume help for one condition covers their other conditions.
Distress and suffering are an existential cornerstone of the human condition, yet how we reflect upon and describe the extremes of our mental duress has varied enormously across history. For more than 100 years, certainly in the West, the predominant means of conceptualizing mental health struggles has been to categorize them… according to hypothetical distinctions between different sets of signs and symptoms…[thus exerting] a profound influence over the ways in which we understand, assess, and manage mental ill health. —PubMed Central
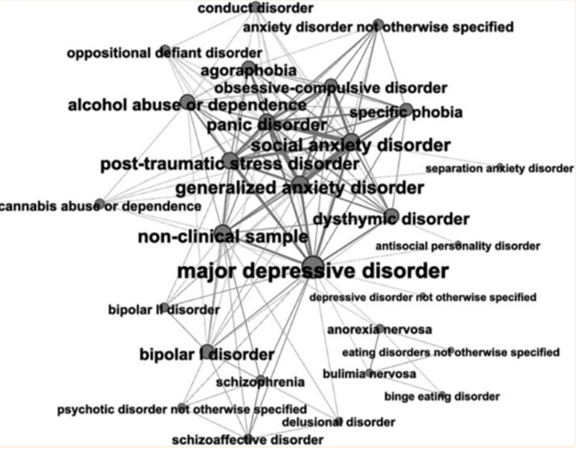
In this network map, each node indicates a specific mental disorder. Node size represents no. of connections with other nodes. Thickness of edge reflects no. of connections between pairs of nodes/mental disorders. From “Transdiagnostic Psychiatry: A Systematic Review,” by Paolo Fusar‐Poli, et al., World Psychiatry. Published PubMed Central/NIH
Coming Up Next

In past posts, I’ve dealt with the origins of autism diagnoses and the birth of the neurodiversity movement. I’m now constitutionally unable to use the word disorder in autism spectrum disorder. Now, I’m mentally removing the D from ADHD, In Post 23: ADHD: Named, Renamed, Still Needs a New Name, I go back to the early 20th century when doctors called it minimal brain dysfunction and clumsy child syndrome — then up through ADHD and into a future of potential name changes to get to something that reflects a condition that recognizes the humanity and not disability of neuroatypical people.
Copyright ©2026 Jan Swan