On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
SYNESTHESIA
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
15. Autism Diagnoses and Behavior Patterns
There’s no way to prevent or cure autism — and there aren’t universal goals to do that anyway. This post moves from diagnosis and symptoms to behaviors and the next two, treatments, treatment controversy, and new research. As we enter a more humane era of neurodivergence, there’s tension among the “treated,” the “treaters,” and the advocates. There are a multitude of sensitivities, but past ignorance or mistakes should not preclude today’s children, adolescents, and young adults from the benefits of early-to-ongoing services and treatments. New treatments have absorbed the lessons from the past, and evidence shows they slow down symptoms, improve behavior and language development, and provide a higher quality of daily life.
I’ve arrived at this is the point of view from the research and stories I’ve read, having no intimate, first-hand experience with autism. I believe the people I know with children, grand-children, and nephews/nieces with autism agree — as long as it’s about the personhood of the individual and not about a disorder that’s freighted with reduced expectations for what they can achieve — and doesn’t underestimate the desire to live independent lives as adults.
Early Autism Diagnosis
Autism is likely a combination of genetic, neurological, and environmental factors. Like many other health issues, the earlier the diagnosis the more likely targeted interventions will help and pave the way for children, teens, and their families in reducing stress, managing resources, and accessing services, as well as lead to better long-term outcomes in school and work.
The Learning Brain and Autism
The benefits of early diagnosis include the opportunity for early intervention, which has been shown to enhance developmental outcomes and improve adaptive skills. Early identification allows for the implementation of specialized interventions tailored to the specific needs of individuals with autism, targeting social communication, language development, and behavioral challenges. Furthermore, early diagnosis enables families to access appropriate support services, educational resources, and community programs, facilitating better coping mechanisms, reducing parental stress, and increasing adult independence. — Chiugo Okoye, et al., “Early Diagnosis of Autism Spectrum Disorder: A Review and Analysis of the Risks and Benefits,” PubMed/NIH
Okoye and colleagues writing in PubMed/NIH caution early diagnosis also entails risks, like the potential for labeling and stigma—with an impact on the child’s self-esteem and social interactions. Another risk is overdiagnosis or misdiagnosis, leading to unnecessary interventions and treatments. They believe in a balanced approach, to consider both the benefits and risks of early diagnosis.
Okoye cites research that’s squarely in the benefits camp. They show how early interventions result in major improvements in children’s social communication when their brains are developing. He gives two explanations —which no doubt would apply to other ND conditions [paraphrased]:

Sensitive periods: Autism develops in specific phases during which the brain is particularly receptive to learning and acquiring skills, due to the brain’s ability to be highly stimulated in early development. In these “sensitive periods,” a child’s learning is highly susceptible to the external environment. The child is more affected by stimuli they’re repeatedly exposed to, which can have a longer-lasting impact on their future behavior.
Neuroplasticity: The brain can reorganize and form new neural connections throughout life, especially ages 2-3. When children with autism are exposed to learning experiences that modify/strengthen neural connections, this “plasticity” (being easily shaped or molded) allows their brains to adapt and reorganize in response. By consistently stimulating the brain, appropriate interventions target and improve cognitive-behavioral functioning and modify the course of autism.
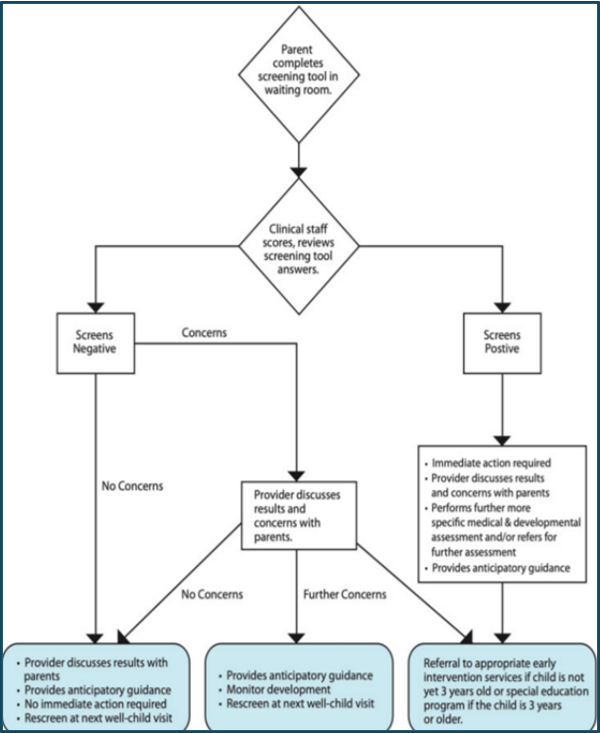
Graphic: Pediatric development screening flowchart, PubMed/NIH
Arriving at a Diagnosis
Here’s what a neuropsychologist looks for or rules out to arrive at an autism diagnosis:
- Shows up early in life: Signs can show up in infancy, like less eye contact, no response to their name, or indifference to caregivers. Others can develop signs after months or years, becoming withdrawn, aggressive, or lose acquired language skills and motor functions. Signs usually are seen by age 2.
- Causes significant impairment: Symptoms vary widely, making it difficult to assess the degree of impairment or ability to function. Clinicians rate impairment from level 1 (minimal support needed) to level 3 (substantial support needed).
- Rules out other causes: Assessments start with medical and psychiatric exams to eliminate other reasons, like developmental delays.
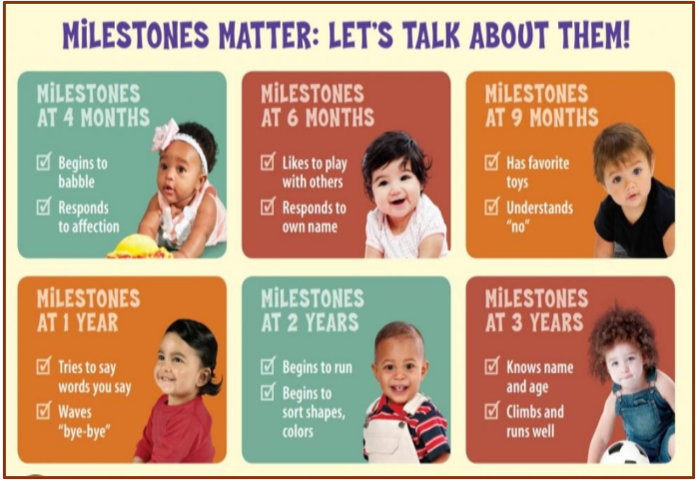
Graphic: CDC.gov/milestones
Some children with autism have difficulty learning, with signs of lower-than-average intelligence. Others have normal to high intelligence—they learn quickly, but have trouble communicating, applying what they know in everyday life, and adjusting to social situations. According to the Mayo Clinic, parents might be the first to notice whether their child:
- Responds with a smile or happy expression by 6 months
- Mimics sounds or facial expressions by 9 months
- Babbles or coos by 12 months
- Gestures—points or waves—by 14 mos.
- Says single words by 16 months
- Plays “make-believe” by 18 months
- Says two-word phrases by 24 months. Retains language/social skills at any age
ASD Symptoms: Social Communication and Interaction
According to the Mayo Clinic, difficulty using language affects how a person with autism perceives, socializes, and communicates with others:
- Doesn’t speak, has delayed speech, or loses previous ability to speak; only starts a conversation to request or label items; fails to respond to name or appears not to hear
- Repeats words or phrases verbatim, without understanding how to use them; doesn’t seem to understand simple questions or directions
- Speaks with an atypical tone or rhythm; may use singsong or robot-like voice
- Has poor eye contact, lacks facial expression; doesn’t express emotions; seems unaware of others’ feelings; resists being held; prefers playing alone, retreating to a private space
- Inappropriately approaches a social interaction by being passive, aggressive, or disruptive
- Has difficulty recognizing nonverbal cues, such as interpreting other people’s facial expressions, body postures, or tone of voice
What Autistic Play Looks Like

“From a young age, autistic kids are likely to line toys up, play by themselves, and repeat actions. They’re less likely to engage in games that require make-believe, collaboration, or verbal communication.” And unlike neurotypical (NT) children who may play this way as well, autistic children are not generally conscious of how others regard their behavior,” writes autism advocate Lisa Jo Rudy, “The Reasons Autistic Children Play Differently,” Very Well Health.
I wanted to include commentary about autistic play for how it defines ND behavior from a very early age. But this passage by Lisa Jo Rudy perked up my attention. It completely describes the way my older son Jaden played as a little boy. Jaden’s ADHD and bipolar disorder certainly cover enough waterfronts, and I’m not looking to affix an autistic diagnoses on top of all that. But it opens questions of these types of behaviors that cross diagnoses. And something I found endearing about my son perhaps deserved another interpretation. The next chart compares autistic and NT play:
Photo: “Why Autistic Children Play Differently,” Very Well Health
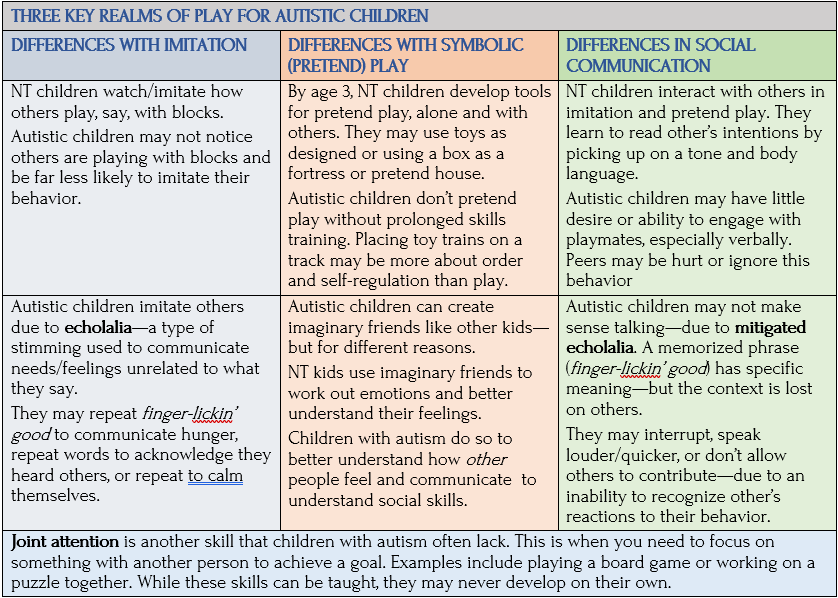
Source: Lisa Jo Rudy, “The Reasons Autistic Children Play Differently,” Very Well Health
According to Rudy, parents of children with autism have noticed these behaviors in play:
- Prefer to play alone, even when encouraged otherwise. They’re happy to toss leaves, sand, or dirt into the air, build up blocks and knock them down, repeatedly complete the same puzzle the same way.
- Don’t/can’t follow rules of shared play, like turn-taking, role-playing, or rules for sports.
- Engage in seemingly purposeless/repetitive play, like opening/closing doors, lining up objects, repeating a phrase from TV.
- Don’t/can’t respond verbally to friendly talk from adults or peers.
- Seem unaware of other children—wandering through a group playing or standing in line.
By ages 2-3, NT children play together and understand sharing, while autistic toddlers generally don’t advance from solitary play or share. They engage in self-regulating activities to manage feelings and avoid becoming overwhelmed, like stimming. Rudy notes that older autistic children see improved skills. They can learn the rules of group play, while still exhibiting different behaviors. In fact, they might focus intently or obsessively on:
- Rules, so that they can’t accommodate any changes (like changing the number of players)
- Playing when others have given up or have turned their attention elsewhere
- Specific features of a game (like football statistics) rather than the game itself
Autistic children are more amenable to parallel play, like coloring or painting, in the same room. It allows them greater freedom in choosing when to talk and allows parents, siblings, and friends to engage and socialize while respecting the child’s needs and boundaries, says Rudy
ASD Symptoms: Patterns of Behavior
When it comes to autism, there’s a distinction between diagnostic symptoms that qualify for a formal diagnosis and behaviors that may be something else (like comorbid symptoms of ADHD or alexithymia — a condition also called emotional blindness) or a reaction to being stigmatized, rejected, or their own recognition of not fitting in. Many autistic children avoid eye contact, but this is more a condition of alexithymia than autism. Research says only around 50% of autistic people avoid eye contact (and not all people who avoid eye contact have autism).
Many with autism have problems with social interaction (less interest or lack of responsiveness, challenges understanding social cues), communications (delayed language development or echolalia, difficulty understanding or using gestures). And many have coordination problems or odd movement patterns, like clumsiness or walking on toes, sometimes exhibiting odd, stiff, or exaggerated body movement.
Stimming Behaviors
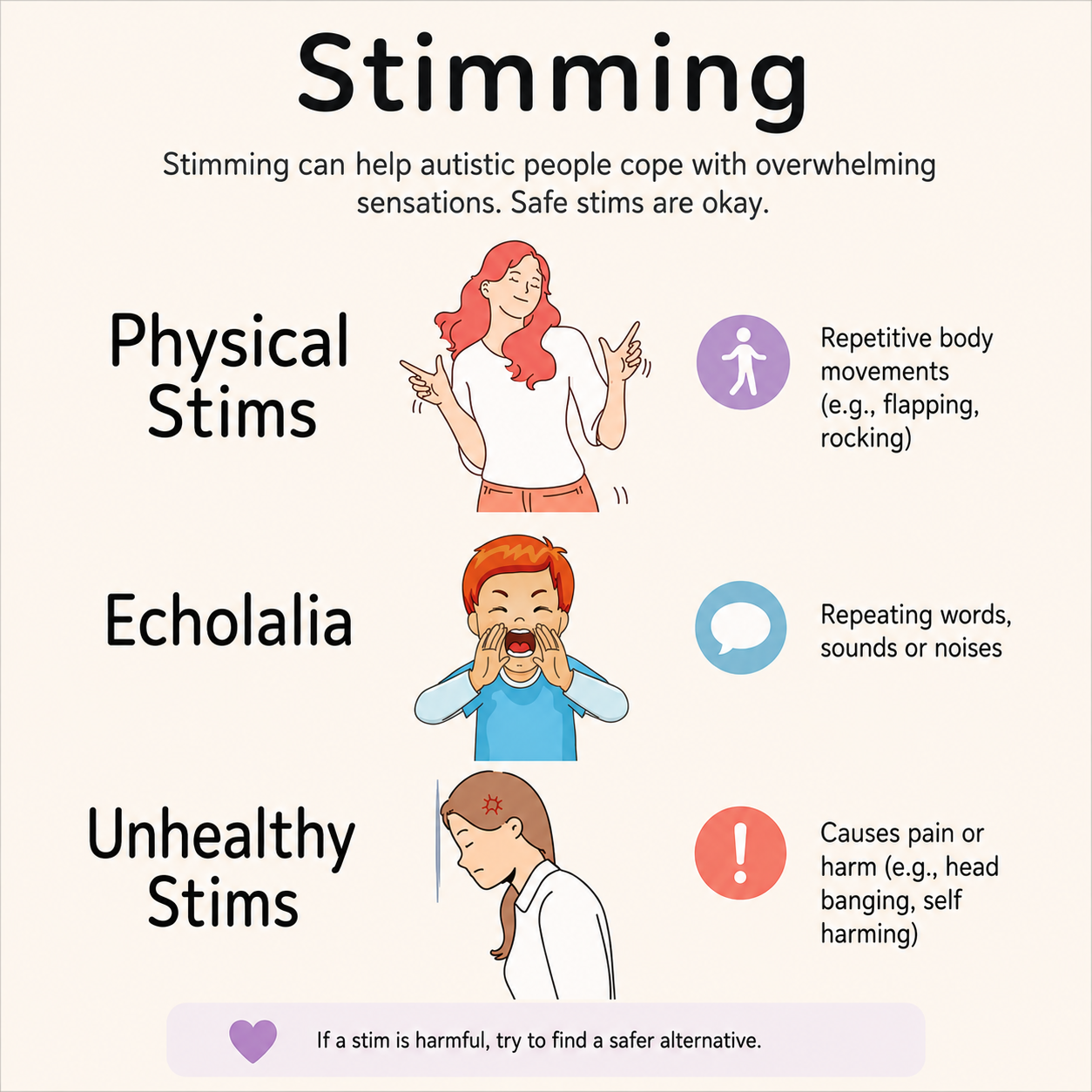
Graphic: NHS Leicestershire Partnership
A significant feature of autism are restricted interests and repetitive patterns of behaviors — or stimming. Stimming, a term evolved from self-stimulatory behaviors, refers to repetitive, stereotyped behaviors — like hand flapping, finger movements, tapping, rocking, spinning, or more harmful behaviors like biting or head banging.
We all can “stim” when anxious, overloaded, or tired. Hair twirling, finger tapping, or leg jiggling relieves stress and distracts from frustration — even reduces physical discomfort. With autism, it’s about the degree of stimming needed.
They might rely on specific routines or rituals and get overly upset at disruption. Or fixate on an object or activity — like a child focused on a toy car’s spinning wheels. Unlike other children, they might not play make-believe or imitate parents.
Autistic people can be unusually sensitive to sensory stimulation — light, sound, touch — while being unaware of pain or temperature change. They may have limited preferences for food, perhaps due to texture or smell or refuse to wear restrictive or clothing perceived as scratchy.
Autism Masking

Photo: Nancy DeVault, “What is Autism Masking,” American Disability
Many with autism understand some of their behaviors, like stimming—are not considered socially acceptable. Autism masking are efforts to suppress or hide “tells” to be more acceptable in a neurotypical world. They may “mirror” NT behavior and develop scripts for social encounters. Tisa Johnson-Hooper gives examples, Henry Ford Health:
- Sound-sensitive adult might try to avoid reacting to loud noises.
- Stimming child might try harder to stop those movements.
- Young adult struggling to understand language might pretend to follow a conversation.
- Teen nervous about asking someone on a date might write a short script to use.
Like anyone, those with autism need to feel accepted by the external world and to find community [see next two posts]. Autism masking can help in the short-term with fitting in and not being judged or ridiculed as “different” — which can boost self-confidence. Therapists can weave masking into therapy that helps individuals rely less on behaviors that have socially ostracized them in the past.
For people with ASD, the pressure to be accepted and meet social expectations can be even more intense because they already feel they have a deficit. Those who rely on masking are more independent, women, teens, and young adults, have been bullied or rejected, and those who want to achieve a goal, like getting a job or making a date.
Unfortunately, when masking becomes part of the daily routine—something people with autism feel they have to sustain—it can come with significant drawbacks. —Tisa Johnson-Hooper, pediatrician and autism specialist, Henry Ford Health

Some of these drawbacks are implications of autism masking over the long term. Johnson-Hooper writes, “When kids with autism use all of their energy to suppress and to hide their authentic selves, there’s nothing left for making social connections, learning, and creative thinking.” Over time, this can lead to stress, anger, and burnout:
- Delayed diagnosis: Suppressing socially unacceptable behaviors can lead to delayed diagnosis and care for some children, particularly those with mild autism.
- Burnout: Hiding natural behaviors or traits can be emotionally, mentally, and physically draining.
- Mental health challenges: Studies suggest adults who camouflage autistic traits are more likely to suffer from depression and anxiety.
Helping People Who Are Masking their Autism
Neurotypicals can’t get inside the mind of someone cracking under pressure of “appearing normal.” But we can relate to the pressure of doing well on an interview, going on a first date, or taking a crowded bus in an unfamiliar city. For those who’re introverted, have social anxiety, ADHD, sensory processing or learning issues, this is also a daily struggle—it’s a relief to get home and take off the mask.
Autism is a complex diagnosis. There are many other diagnoses with similar features. So even people who haven’t been diagnosed with autism may engage in masking behaviors. —Tisa Johnson-Hooper, pediatrician/autism specialist, Henry Ford Health

Here are Johnson-Hooper’s recommendations for helping someone you care about with ASD or other neurological difference better navigate the world [paraphrased for brevity]:
- Show acceptance, so they know they don’t have to hide their true selves with you and that they’re worthy of love and acceptance.
- Don’t take outbursts personally. Autism masking to meet social demands can make them irritable, volatile, or anxious—they may need a release after holding it together all day.
- Prepare a social script, to help them find ways to minimize the energy required for masking, so they have something to say in different social settings.
- Think of workarounds. Children stimming to calm down may benefit from more acceptable toys, like a fidget spinner or wobble chair. Knitting or doodling can keep hands busy.
Coming Up Next

Autism interventions, as seen through a neurodiversity lens, have become controversial. I’ll devote Post 16: Autism Treatments that Help to treatment options, tailored to age, severity, and other needs. I’ll follow this with an excerpt of writing by an extraordinary young man with autism who can only recently communicate through his writing.
Copyright ©2026 Jan Swan