On Neurodivergence and Otherness
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions — Part I
7. A Synthesis: Sensory Systems and our Emotions — Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
SYNESTHESIA
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry — Part I
12. Synesthesia, Creativity, Artistry — Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive … and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Complexity, Clarity, and Self
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Empathy Recognizes and Navigates Difference
41. Reducing Neurotypical-on-Neuroatypical Conflict – Part I
42. Reducing Neurotypical-on-Neuroatypical Conflict – Part II
43. Communicating Across the Neurospectrum – Part I
44. Communicating Across the Neurospectrum – Part II
45. Neurodiversity: Advocacy and Education
46. Neuroinclusion in the Workplace
47. A Neurodiverse Lifestyle
IN CONCLUSION
48. In Conclusion: Neurodivergence and Inspiration
8. Sensory Disorders and Sensitivities

So, as we learned in post 2, there are definitely 7, 8, 10, 21, or 33 senses altogether. A real head scratcher. As we shift from sensory systems that work more or less as they should (neurotypicals) to those misfiring, jamming, melting down, or heating up (neuroatypicals), we arrive at equally murky waters. Researchers are only recently learning the reasons why and then what to do about it for sensory disturbances and troubling effects on mental health.
Disrupted senses limit how we interact with others, our environment, or our ability to perform, says Hardeep Ranu, PhD, research project manager for Harvard Catalyst. Examples:
- Hearing loss makes it harder to be in conversations, especially in noisy situations. Tuning out repeatedly over time can reduce mental acuity.
- Reduced vision makes driving impossible and limits independence.
- Balance disorders cause falls and physical calamity or, at the least, limit safe movement.
- Proprioceptive curtailment limits ability to move without carefully observing hands or feet.
- Vestibular disequilibrium throws off a sense of balance and causes vertigo, increasing the likelihood of feeling uneasy in unfamiliar spaces.
Ranu summarizes impressive research studies looking at possible non-invasive, safe, and drug-free treatments for these and other sensory challenges, from Harvard’s Five Senses: Input & Response program, Harvard Medical School teaching hospitals [edited for brevity]:

Source: Hardeep Ranu, Harvard Catalyst
Sensory Impairment in Aging Adults
A strong body of evidence finds sensory impairment affects mental health. People with multiple impaired senses experienced more loneliness and had significantly worse, overall mental health. People with three sensory impairments were more likely to experience frequent depressive episodes. So report researchers at UChicago Medicine. They analyzed data on sensory function (vision, hearing, smell) and self-reported mental health from 4,000 older adults collected over 10 years, as part of the National Social Life, Health & Aging Project.
Of the three senses studied, vision impairment caused the greatest distress. Older people with poor vision may have trouble getting out of the house or seeing the faces of friends and family. Hearing loss can make conversations stilted and frustrating. Even loss of smell affects their ability to find joy in familiar scents—like a favorite home-cooked meal. Older people felt stigmatized by these diminished capacities.
In the face of that stigma, the researchers say their results highlight the importance of improving access to mental health services and increasing awareness of the connection between sensory loss and mental distress. In particular, understanding how different sensory disabilities impact the long-term mental health of older adults could help healthcare professionals … screen for mental health conditions when they identify sensory loss in their patients, providing opportunities for personalized and timely interventions. —Grace Niewijk, “Declining Senses Can Impact Mental Health and Loneliness in Aging Adults,” UChicago Medicine, 2024
In addition to proactively treating older adults’ mental health, researchers suggested ways to lessen daily effects of sensory difficulties — which in turn lessens impact on mental health.
Sensory Processing Disorder (SPD)
In a prior post, I covered sensory processing as the body’s way of organizing, interpreting, and prioritizing information for the brain to respond—and how this influences the body’s ability to be in harmony with itself, move in space, and interact with the physical and social world.
When it doesn’t quite work like this, it could be an indication of sensory processing disorder (SPD), a neurological condition in which the brain can’t intelligibly process multisensory inputs. SPD can affect any combination of senses, including sight, hearing, touch, taste, smell, balance, and body awareness. Especially children can have a hard time meeting the demands of body and environment — in schoolwork, play, sports, work, relating to others (in groups), and dealing with stressors, like loud noise, bright lights, or crowds.

Graphic: Dreamstime
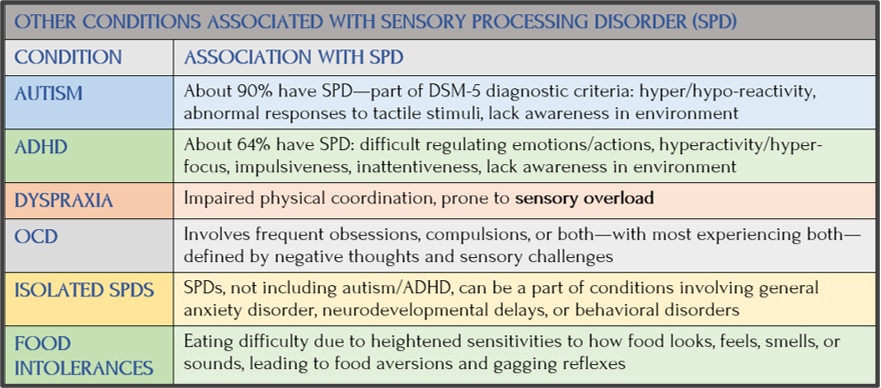
When my son Etan was little, he was diagnosed with sensory integration dysfunction (SID), SPD’s precursor. Yet, for the past 15 years, SPDs are only documented as part of other disorders in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5). SPD patterns are also described in the Diagnostic Classification of Mental Health and Developmental Disorders in Infancy and Early Childhood or DC:0-5 (like DSM-5, revised in 2014). Many adults and parents of children with sensory challenges argue for SPD as a standalone condition — with no other diagnosis — to be treated as such. For now, SPD is co-occurring with other disorders:
sensory integration
Jean Ayres, Facebook
Occupational therapist A. Jean Ayres identified sensory integration issues in the 1970s. Wikipedia says Ayres studied people whose brains didn’t automatically integrate sensory stimuli to respond properly, adding to their everyday challenges. She added to the five special senses the two internal senses of body awareness (proprioception) and movement (vestibular) .
According to two studies, there are measurable neurological differences between children with SPD, children classified as neurotypical, and children diagnosed with autism. Despite no consensus on SPD as a disorder or how it’s diagnosed/treated, the question is to whether SPD should be treated or just seen as different. This is tricky. As the mother of a diagnosed with SPD when still toddling about—I’m squarely in the “let’s fix it to-the-degree-possible” camp.
Etan’s Sensory Processing Disorder (SPD)
I’ll talk about Etan later, but just a word on his SPD. I knew his fine/gross motor skills delays were past normal ranges. But I didn’t discover SPD was a thing until he was assessed, as suggested by his nursery school director. For example:
- Washing hands: If you’ve never thought about steps to complete handwashing from lathering up to rinsing off, then you don’t have SPD. For 4-yo Etan, he might grab the dry soap in his dry hands, pause to consider, put the soap back down, turn on the water and then proceed with more confidence. Not an automatic process.


- In the playground: He climbed the jungle gym, but at the top of the ladder could not go further or climb back down, like a pussycat up a tree. His buddies scampered all over the place, moving around my son frozen in place until rescued.
- Walking in the woods: Either he avoided the branch hitting his face or stepped over the protruding root on the path, but not both. One proprioceptive stimulus at a time.
- Swings and bikes: Most little kids sense the body motion to swing or ride a two-wheeler. Etan was two biological years behind his age group before mastery. His schoolmates compensated for his delays —they pushed him on the swings and helped him put on his winter jacket. Pretty cute.

More on Sensory Processing Disorder

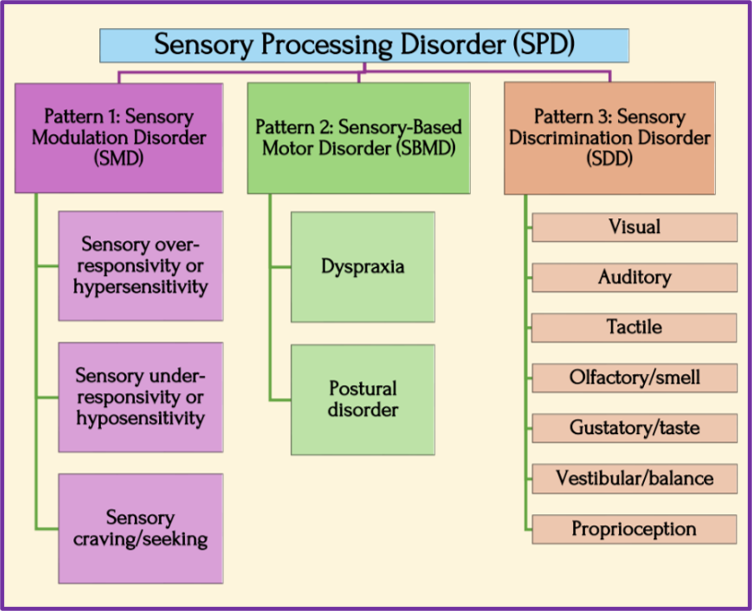
Because neuropsychiatry hasn’t agreed to SPD as a distinct condition — apart from underlying symptoms of other disorders — there’s not one taxonomy of categories and characteristics. Wikipedia’s page documents four different models. The one with three “patterns” (see below) is corroborated by Sensory Health and Child Mind Institute—showing SPD reveals itself in many complex and varied ways.
According to the PubMed Central/NIH journal Brain Science, SPDs are conditions when common stimuli have difficulty “detecting, modulating, interpreting, and/or responding to sensory experiences.” Sensory receptors malfunction, so bright or flickering lights are too bright, noises are too loud, textures chafe or scratch, shoes are too tight and uncomfortable.
This condition leads to symptoms being misperceived as clumsiness, slowness, or an inability to climb stairs, tie shoes, or button a shirt.
Source: Living Compass
However, as writer Beth Arky described in her Child Mind Institute post, very young children can exhibit extreme behaviors at the higher end of the SPD spectrum, indicating they’re overwhelmed and confused:
- Screaming if forced to wash their face or throwing tantrums when forced to dress
- Having an unusually high or low pain threshold; crashing into walls and even people
- Putting inedible things, including rocks and paint, in their mouths
Arky believes it would help parents to understand this about their kids:
- Dramatic mood swings and tantrums: A child’s outsized reaction to change occurs once overloaded by visual and auditory stimulation. Arky’s example is the difference between a first grader calmly listening to a teacher reading a book but losing it in a grocery store.
- Fight-or-flight response (FFR): A child reacting to something upsetting—often not detected by the adult—can suddenly flee from the stimulus and to danger, like running out the front door into the street. Or, to a calming sensation, to a secret place where the child feels safe.
- Aggressive behavior: Aggression is a common reaction to sensory overload. “They’re having a neurological panic response to everyday sensations the rest of us take for granted.”
All young children learn emotional self-regulation as they grow and develop, but a child with SPD would find it challenging to prioritize self-regulation and safe behavior over “their need to get that input or that calming experience.”
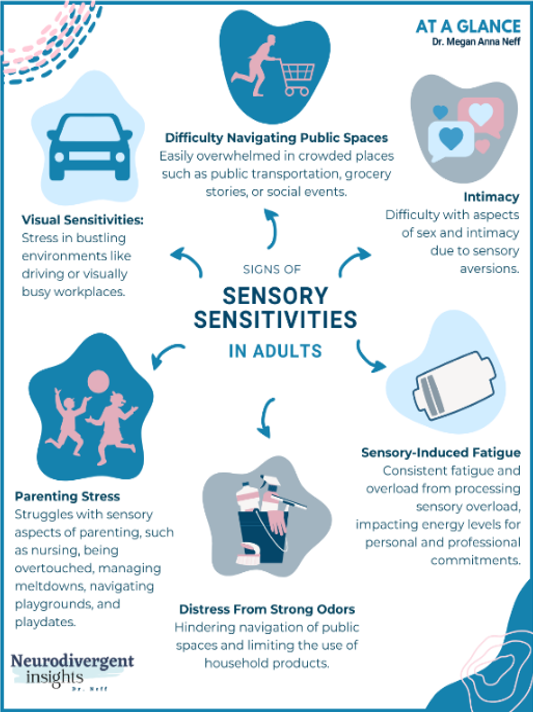
SPD is Common in Neurodivergent Adults
SPD can affect multiple senses in varying ways and intensities. Neurodivergent and neurotypical adults can both have sensory processing difficulties, as seen in this three-3-pattern SPD model.
Pattern 1: Sensory Modulation Disorder (SMD)
Sensory modulation disorder (SMD) changes neural messages conveying information about the intensity, frequency, duration, complexity, and novelty of sensory stimuli. It has three subtypes:
- Sensory over-responsivity (hyper-sensitivity or sensory defensiveness) causes people to be easily overwhelmed by sensory stimuli. This can even trigger the body’s fight-or-flight response [see anxiety post 5 on FFR] — causing them to act aggressively or withdraw. Other signs are intolerance for bright lights, loud noises, fabric/food textures, being unexpectedly touched. They’re not aware of their body in relation to people/objects or don’t sense their power (slamming objects down).
- Sensory under-responsivity (hyposensitivity) is the opposite, with people withdrawn/hard to engage or self-absorbed because of poor detection of environmental sensory input. Being under-response to tactile pressure leads to poor body awareness, clumsiness, or movement with too much/too little force. They may not perceive anything too hot/too cold or painful. Many hyposensitive people seek sensory stimulation, as in constantly touching people or textures, without understanding personal space or what’s socially unacceptable.
- Sensory craving/seeking is fidgeting, impulsiveness, seeking or making loud, disturbing noises. People with this pattern also have sensorimotor-based problems, including slow, uncoordinated movements or poor handwriting—made notable by an almost insatiable desire for sensory stimulation. They are constantly moving, crashing, bumping, and/or jumping. They may “need” to touch everything and be overly affectionate. Sensory seekers are often thought to have ADHD.
Graphic: Megan Anna Neff, Neurodivergent Insights
Pattern 2: Sensory-Based Motor Disorder (SBMD)
People with SBMD have disorganized motor movements from poor sensory processing, affecting the stability of their bodies and their ability to handle physical tasks. It has two subtypes:
- Dyspraxia (developmental coordination disorder, DCD, or motor planning problems) cause individuals to have motor planning problems and other sensory processing challenges. They may have difficulty in forming a goal or idea, planning a sequence of actions, or performing new motor tasks. They can be clumsy, awkward, and accident-prone — with poor skills in sports or tasks requiring fine motor skills. Those with DCD may prefer sedentary activities or mask motor planning problems by videogame play.
- Postural disorder causes individuals to have difficulty stabilizing their bodies to control movement. When postural control is good, individuals can reach, push, and pull, with good resistance against force. Those with poor postural control often have difficulty maintaining a good standing or sitting position.
Pattern 3: Sensory-Discrimination Disorder (SDD)
SDD causes individuals to struggle with attributing correct qualities and meaning to sensory stimuli — inaccurately “reading” what they see, hear, feel, or sense in movement or balance — as well as difficulty detecting similarities and differences among stimuli, as in discerning letters or hearing words, feeling and recognizing shapes not seen, falling to the side or backwards, or dropping things. Individuals with SDD may appear awkward in both gross and fine motor abilities and/or inattentive to people and objects in their environment. They may take extra time to process sensory stimuli from the special senses.
Prosopagnosia
While not a sensory disorder, a neuro-cognitive condition, called prosopagnosia or “face blindness,” is worth a brief mention. According to the Cleveland Clinic, people with prosopagnosia can’t recognize faces or facial expressions—rather their brains can’t. It falls under a family of conditions, agnosias, which interfere with how the brain processes information from the senses. Famous “sufferers” of face blindness are two world-renowned scientists: in conservation, Jane Goodall, and in neurology, Oliver Sachs.
And it affects one unfamous person, my son Jaden. In his telling, he can’t recognize characters in a movie if they change their clothes, or they disappear for several scenes and then reappear. He’s a bit better in person, but not great at remembering people he hasn’t seen for a long time.

Prosopagnosia qualifies as a neurodivergent condition for the reasons Goodall makes clear in her meditation on her neurodisorder (from Sparrow Rose Jone’s blog, Face Blind):
During my travels, one thing detracts from my enjoyment of meeting people. I suffer from an embarrassing, curiously humbling neurological condition called prosopagnosia, which, translated, means I have problems in face recognition. I used to think it was due to some mental laziness, and I tried desperately to memorize the faces of people I met so that, if I saw them the next day, I would recognize them. I had no trouble with those who had obvious physical characteristics — unusual bone structure, beaky nose, extreme beauty, or the opposite. But with other faces I failed, miserably. Sometimes I knew that people were upset when I did not immediately recognize them — certainly I was. And because I was embarrassed, I kept it to myself.
Quite by chance … I discovered my own sister, Judy, knew similar embarrassment … I wrote to the well-known neurologist Dr. Oliver Sacks. Had he ever heard of such an unusual condition? Not only had he heard of it — he suffered from it himself! And his situation was far more extreme than mine ….
Even now that I know I need not feel guilty, it is still difficult to know how to cope — I can hardly go ’round telling everyone I meet that I probably won’t know them from Adam the next time I see them! Or maybe I should? It is humiliating, because most people simply think I’m making an elaborate excuse for my failure to recognize them and that, obviously, I don’t really care about them at all — so they are hurt. I have to cope as best I can — usually by pretending to recognize everyone! And while that can have its awkward moments too, it’s not nearly as bad as the other way around. —Jane Goodall, Reason for Hope: A Spiritual Journey, co-author Phillip Berman (1999)
Coming Up Next
In Post 9: Etan’s Story, I’ll return to SPD through a profile of my son Etan. Sometimes I wonder why so many in my family (including me) are afflicted with one thing after another. Though not at all helpful, I do sometimes feel sorry for my sons, whose mental disorders have made life a complicated struggle. Now in their thirties, I see their maturity, grit, and talent are helping them make their way. There’s reason for optimism. I’m bullish on the subject of neurodiversity. Those who are vulnerable, bullied, isolated — we just have to do better as a society.
Copyright ©2026 Jan Swan