On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
Anxiety is treatable. That’s the headline — and it’s more important than most of us realize when we’re in the middle of it. Of course, knowing that isn’t the same as knowing what to do about it.
I often think I get lost driving at the first turn out of the side street, going left when I should’ve gone right. Knowing where to start and who to trust can be the first correct turns in moving toward what actually helps — instead of what just adds more noise or, to continue the metaphor, gets us hopelessly lost.
In this post, I give expert opinions about the well-traveled road to effective treatment: how to find support, how to work with professionals, how to stay engaged long enough for something to change.
There are numerous individualized therapies designed to meet our needs, to teach cognitive and behavioral life skills, and to simply reduce overwhelming, persistent stress and anxiety to live a more peaceful, less encumbered life.
Hiroshi Sugimoto, Plum Estate, Kameido, 1858
Sources for the following recommendations: Kripa Balaram and Raman Marwaha, NIH National Library of Medicine; psychiatrist Sandra Swantek, Chicago, and psychiatric resident Nicholas Fletcher, Detroit, AMA podcast; and other sources
A Guided Experience
So much is now known about how mental and physical health are inherently related. We just have to look at all our symptoms (or our child’s) to know when it’s time to seek a medical/health professional’s help. We need to consider — and not dismiss — signs like excessive worry, irritability, trouble with drinking or drug use, trouble sleeping, irritable bowel syndrome (IBS), or other noteworthy behavior changes. First, medical doctors need to rule out medical causes for anxiety, like thyroid problems, hypoglycemia, hormone imbalances, heart disease, asthma — or interacting drugs and supplements, including prescriptions, over-the-counter medications, herbal remedies, and/or recreational drugs.This the part that can feel overwhelming — appointments, decisions, unfamiliar roles, too much information at once. It helps to think of it less as steadily figuring everything out and more as building a working relationship with care.
Get emotional support.
We need our family and close friends to help us work through our fears. Support or therapy groups help connect us with people who are going through the same things. Fight the inclination not to seek help. Offer support in return — that will make you feel positive about giving back.
Anxiety is normal. Anxiety is a part of getting ready for an intense situation sometimes. But when you find yourself avoiding situations, it’s having an impact on your relationships with people, and you’re avoiding things you need to do to be functional and successful and move through life in a positive way—all these things are signs that it’s probably time for you to get some help.” —Psychiatrist Resident Nicolas Fletcher, Authority Health, Detroit, in American Medical Association NewsWire podcast
I have a friend I met in a therapy group nearly 20 years ago. We both have children with complicated psychiatric conditions and, even though the group ended long ago, our friendship endures.
But we’re also the friends who text “I need a consult.” What that means is we jump on the phone to listen and problem-solve together. We’re both savvy enough to recognize there are no quick solutions, because if there were we would have tried them. Our friendship, now separated by three states, is a lifeline.
Get help early.
Early diagnosis and treatment help reduce symptoms and prevent anxiety conditions from getting worse. This is advice for almost any condition, as in: take migraine meds before it gets so bad you can barely see. Get cancer screenings to treat in stages 1 or 2, instead of stages 3 or 4. While our instinct may be to deny, mask, withdraw, or otherwise procrastinate, we must apply the brakes before it’s a runaway train.
Get professional help.

Photo: Vecteezy
So much is now known about how mental and physical health are inherently related. We need to look at all our symptoms (or our child’s) to know when it’s time to seek a medical/psychiatric professional’s help. This includes considering — and not dismissing — signs like excessive worry, irritability, trouble with substance use, trouble sleeping, irritable bowel syndrome (IBS), or other noteworthy behavior changes.
Medical doctors can rule out medical causes for anxiety, like thyroid problems, hypoglycemia, hormone imbalances, heart disease, asthma — or interacting drugs and supplements, including prescriptions, over-the-counter medications, herbal remedies, and/or recreational drugs.
Psychotherapists or other clinicians can work with us to determine the cause and type of our disorder, help us address the anxiety, and customize care to prevent anxiety-related illness. Steps:
- See a medical doctor first. Before the first visit, especially if shy or nervous, it’s a good idea to write down questions. If possible, give the reason for the visit — and desired outcome. Doctors can also recommend psychiatrists for meds and psychiatrists can recommend psychologists, social workers, and others for therapy.
- If you see a psychiatrist for meds, know what is being prescribed, their benefits, side effects, alternative treatments — and why any tests and procedures are recommended and what the results could mean. Know what to expect if you refuse medication or tests/procedures.
- First visit with a therapist (go for a psychotherapist for severe anxiety) should assess fit. I can’t imagine seeing someone I don’t instinctively trust and believe in. I also recommend taking notes, because it’s difficult to process what we’re hearing about our diagnosis, meds, or treatments on the spot.
- In-person vs online: I wouldn’t advise online therapy with someone you haven’t met in person. I see my therapist online now, but that’s after ten years of seeing him in person. But if online is the only way, seek trusted sources for recommendations, like Psychology Today.
- Understand the purpose of follow-up appointments, and make sure you have all the contact information. This may sound too obvious for words. My son with bipolar disorder [I write about him in my bipolar series] missed a decade of medical history because he never obtained copies of his records. He has little recollection of doctors and therapists he has seen or where he was when treated. We need this information. HIPAA laws are strict, so each of us has to do this for ourselves or for a dependent child.
- Therapists are guides. But they can’t accomplish positive outcomes without our active participation. It’s actually hard work, and sometimes we feel worse after therapy than better. Sometimes there’s little discernable progress. But then there’s a leap in insight.

Image: Spring Health
Looking backwards, it’s hard to recognize ourselves. Keep appointments. If too frequent, slow them down. Take breaks if needed, but first discuss.
- Medications: I’m a believer. If you go this route, there’s plenty of trial and error. But it’s worth it when you land on the right prescription/s. Take as directed, not more or less.
Manage anxiety and stress.
I’ll talk more about this in post 17. It’s a good life skill to learn how to calm ourselves and find relaxation techniques that work.
- Learn coping skills in psychotherapy and alternative programs, to gain confidence, curb embarrassment, worry, or panic, and improve our ability to interact with others.
- Identify the severity of the anxiety disorder or level of impairment or distress it causes in our life. Mild or moderate symptoms might be a choice between psychotherapy and pharmacotherapy. Severe symptoms might require a combination of therapies and medication/s to achieve adequate symptom management.
- Think about triggers — what’s causing stress/anxiety — and note whether we avoid certain people, situations, or places. That gives a lot more information about the source of our fear.
Commit to the treatment plan.
This helps prevent relapses or worsening of symptoms. Together with our therapist, we can choose the best path toward symptom management.
- Cognitive-behavioral therapy (CBT) is an effective, evidence-based treatment addressing and relieving targeted symptoms, lessening other symptoms, and improving quality of life.
- For agoraphobia and panic disorders, there’s data suggesting combining CBT with pharmacotherapy may be the most effective treatment. According to DSM-5, remission rates without treatment are quite low, with averages estimated at about 10%.
There are many other therapies. I’ll touch on a few later.
Working through anxiety takes time.
You didn’t get here overnight. Whatever you’ve been going through is something you’ve probably been dealing with for quite some time, and it’s only now that you’re here. With that in mind, I don’t have a pill or anything that’s going to fix it overnight. Studies show, even with medication, it can take anywhere from six months to two years before you’re able to live a better life with your anxiety. Because what has happened is over that time period, you have learned what it is about the anxiety that leads it into a disorder. You’re essentially getting a better understanding of yourself and what your triggers are. —Psychiatrist Nicholas Fletcher, American Medical Association NewsWire podcast
Treatment Options
In today’s world of many new approaches to treatment, from minimally invasive to surgical, it can be tough to find the right treatment — and how anxiety affects our daily life. It may take trial and error to discover what works best: long-term psychotherapy, short-term CBT, newer variants of CBT, family therapy, combinations of approaches, individual vs group therapy, led by psychotherapist vs clinical social worker, medication cocktails — and the list of variables continues.
In the next posts, I’ll discuss many options, traditional and nontraditional. For some people, talk therapy is all they need. For others, they want the structure of CBT. Almost no one recommends just medication — always in combination with a form of therapy. For me, it’s individual and group psychotherapy plus medication — without all this and my commitment to it, I believe my life would be so much more stressful and less manageable.
Enhancing Healthcare Team Outcomes
Whether we’ve been diagnosed with GAD or agoraphobia, we know now it gets worse without treatment. Sadly, that’s a challenge for someone who might be functioning at half mast, has trust issues with the medical community, lives far from psychiatric help facilities, finds the costs and lack of insurance daunting, and doesn’t know what they need — a sufficient number of barriers for even the most knowing among us.
How are we to find healthcare professionals who are experienced in diagnosing and producing treatment plans for our specific issues and well-versed in the symptoms and treatments for phobias, agoraphobia, and panic attacks? And quickly?

For more severe problems, like panic disorder, we may need more than one well-intentioned therapist. We might need a team, what the health field calls interprofessional interventions: of psychotherapists, psychiatrists, and medical doctors. Or maybe social workers, psychiatric nurses, and nurse practitioners. Together they participate in and monitor education and care. Don’t ignore:
- Nursing staff, who can assess compliance, answer questions, and watch for adverse effects from medication, alerting the prescriber promptly of any concerns. They can also be very accessible, empathic caregivers.
- Pharmacists, who review prescriptions, check for interactions, and inform patients about side effects. They can also provide input on which agents are best to use for a specific patient and therapy modifications if progress stalls.
All of this assumes something that isn’t always true — that care is accessible, coordinated, and easy to enter. For many people, it isn’t. The next challenge is not choosing treatment. It’s finding and sustaining it.
Cognitive Distortion, Negative Thought, Automatic Thought
Before concluding this post and moving on to treatments for anxiety disorders, I’d like to talk about an aspect of anxiety we probably have all experienced time to time. For those with anxiety disorders or serious mood disorders, it’s probably more frequent and ongoing than not: and that is, automatic, negative, biased, and illogical thinking patterns that bring us down and make us believe the worst about ourselves and the world in which we live. As follows:
Cognitive Distortions
Cognitive distortions, also referred to as automatic or inaccurate thoughts, are interdependent with stressful or distressing emotions. In normal situations, we can turn negative based on how we interpret our view of reality. If we see things through the lens of inaccurate, biased, illogical, or distorted thinking, we can easily form bad (maladaptive) habits of thinking this way all the time. This clearly worsens our anxiety and depression, since emotional responses to situations arise from how they are perceived. There are two kinds of distortion:
- Tangible distortion: We believe we can’t complete something despite clear evidence to the contrary. Or, we believe we’re having a health emergency, even though our doctor just gave us a clean bill of health.
- Abstract distortion: We believe we’re disliked by our friends or not loved by our significant other. We might believe we’ve permanently lost a core aspect of our identity or personality.
Examples of cognitive distortions:
- Black-and-white or “polarizing” thinking: We tend to see something as all good or bad. To reinforce this, we refuse to see nuance or complexity. I’m perfect, or I’m a total failure. We use words like always, never, impossible, or disaster. Negative polarizing thinking is particularly destructive to our senses of self and our relationships.
- Catastrophizing: Here we assume the absolute worst possible outcome in any stressful situation, or we exaggerate the insurmountable difficulties to be faced. We think we’ll fail an exam and therefore are losers at life. Some catastrophizing is unintentional, more than merely over-exaggeration. It can result in high frustration, anger, and low self-esteem.
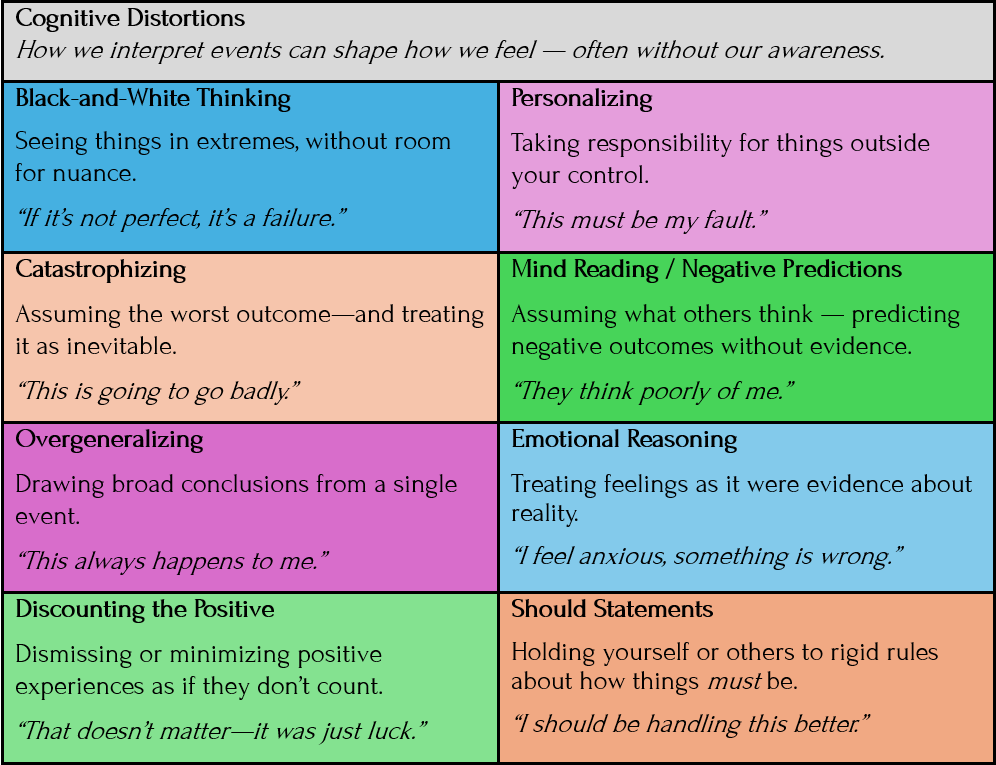
- Overgeneralizing: We are overly broad in how we perceive events or people. We use words like always, never, everybody, and nobody—despite their lack of accuracy. Once something “always” happens, we see a pattern of events, not just one event. I “always” get stuck at “every” red light makes me frustrated every time I get in the car. I keep myself in an angry state, express anger in less healthy ways, and suffer greater consequences as a result.
- Personalizing: We automatically blame ourselves, despite evidence a situation is not our fault or is beyond our control. If no one responds to a group text, it’s not because we’ve lost our friends. It has nothing to do with us—perhaps they’re busy or missed the text. Or, like me, forgot. We’ve wasted psychic energy on someone who is not thinking about us at all.
Negative Thoughts
Negative thinking contributes to nearly all anxiety problems, especially social anxiety disorder (SAD), depression, stress, and low self-esteem. Therapists describe negative thinking as:
- Unrealistic attributions: We make decisions or come to conclusions about why something happened that is simply not true or accurate.
- Unrealistic expectations: We assume a level of control we don’t have in a situation, causing us to be disappointed when our expectations aren’t met.
- Predicted outcomes: We meet someone new and try to figure out (“predict”) the positives or negatives of a potential relationship. A positive prediction may lead us to increased attraction, but a negative prediction can be self-fulfilling and end in a non-relationship.
- Internalized defectiveness schemas: We have feelings of being “defective” or bad, unwanted or inferior in important ways or, if exposed, being unlovable to significant others. This one hurts, like someone read my journals.
Throughout my young adult life, I harbored secret thoughts it was just a matter of time until my boyfriends, friends, coworkers, and general acquaintances would realize who I was, and I’d be ghosted, gaslit — annihilated. Even today, these feelings creep in, until I banish them. What we do to ourselves!
Coming Up Next

In Post 15: Treatment Options for Anxiety Disorders — Part I, I’ll begin discussing treatment options for anxiety disorders, from the traditional to the less traditional. Our therapists can help us choose what seems right for us.