On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
10. Specific Phobias and Agoraphobia

Fear of snakes, called ophidiophobia, is thought to be the second most commonly reported animal phobia, according to Heather Hall, “The Big List of Animal Phobias,” A-Z Animals Photo: Willem Van Zyl / Shutterstock.com
There used to be three distinct but related conditions when it came to phobias. But much has changed in the way they’re now classified, based on new research and clinical insights. Still remaining a phobia condition, specific phobias are a collection of individualized phobic fears with enough commonalities to be grouped together. The other former phobia is agoraphobia, now classified in its own unique category. The third, historically called social phobia, is now folded under social anxiety disorder [post 7] — though I still discuss it as having some phobia characteristics.
In her article, “5 Common Effects of Phobias on Your Emotions and Personality,” VeryWellMind, health writer Lisa Fritscher providesexamples of how phobias can compound the overwhelming emotions triggered by the fear with anxiety, loneliness, embarrassment, and feelings of helplessness and despair [paraphrased; changed “you” to “we/us”]:
- Life-limiting and severe anxiety: Depending on the phobia, we might struggle to live a normal life at work or school, with friends and family, or pursuing our interests.
- Isolation: Experiencing social isolation resulting from a phobia accentuates our differences and not commonalities with others. This affects our relationships by keeping close people at a distance—causing us to become more depressed and reclusive.
- Embarrassment: Being phobic can create awkward or embarrassing situations. Like having to beg off from going to our friends’ house because we fear their dog or fear being humiliated at a party, convinced we’re the subject of gossip.
- Feeling out of control: Despite understanding our phobia is irrational and excessive, we’re emotionally distraught we can’t get it under control. We think of what our life might be like if we could just stop feeling dread at encountering what we fear.
- Helplessness: When we realize our phobia is affecting our relationships and job, as well as our sense of wellbeing, we feel helpless — like there’s nothing to do to heal. We wish things were different, but feel they’ll never be.
Specific Phobias

Photo: “Exposure Therapy: How It Works to Treat Anxiety and Fear,” ReachLink
Formerly called simple phobia, specific phobia is characterized by sharp, persistent fear of specific objects, activities, or situations posing little real danger. But for those of us experiencing these phobias, these fears are real enough. We find our reactions come up fast and sharp, without forethought there we are — overwhelmed, afraid, and backing away. Our fears are mostly unreasonable, even if we can trace their origins, and stubbornly persistent — unless we seek professional help. Otherwise, most of us live our lives through avoidance. If the fear is manageable (I’m claustrophobic and don’t like crowded elevators — but I still take them), then we just live our lives with this annoyance that flairs up on occasion. If, however, we take 25 flights of stairs to avoid the elevator, then avoidance is not a great idea.
Specific Phobias Types and Risk Factors
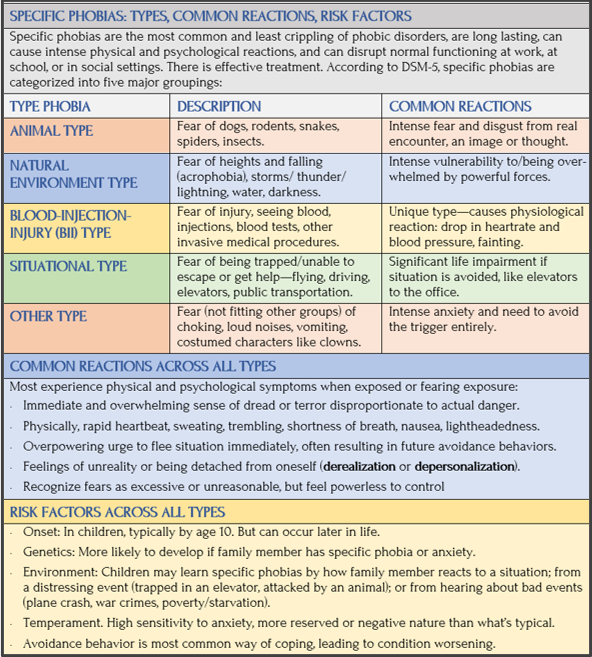
Sources: Mayo Clinic, Very Well Mind
Group Splitting: The Evolutionary Advantage of Specific Phobias
Danger may give rise to fight or flight or freezing or jealousy or washing or checking or to the construction of fall-out shelters, and all of these activities are accompanied by the dysphoric affect of anxiety ….
In avoidance of aspects of the habitat, such as cliffs and caves, one must suspect that anxiety may have had a function in the splitting of early human groups, as acrophobics abandoned communities living on cliff tops and claustrophobics abandoned communities living in caves. —Psychotherapist Hilary Jacobs Hendel, NAMI blog
- Immediate and overwhelming sense of dread or terror disproportionate to actual danger.
- Physical: rapid heartbeat, sweating, trembling, shortness of breath, nausea, lightheadedness.
- Overpowering urge to flee situation immediately, often resulting in future avoidance behaviors.
- Feelings of unreality or being detached from oneself (derealization or depersonalization).
- Recognize fears as excessive or unreasonable, but feel powerless to control
Hendel sees this concept of “group-splitting” by phobia as a variable in behavioral ecology, with implications for the evolution of natural selection at the group level.
What do you fear the most? Heights? Tight places? Desert-dwelling black widow spiders or jungle-dwelling boa constrictors? Perhaps the ancient clan we’re descended from is the reason we have this fear.
One Person’s Thrill is Another’s Horror
Image: Shutterstock
Horror films and heights have a dividing effect. Some feel thrilled and energized by having their wits scared out of them or by leaning over the Guggenheim Museum’s parapet at the top of the spiral, while others recoil in genuine fear.
My boyfriend and I were walking on a path along a cliff edge overlooking the ocean. I went closer to the edge and when I turned around to tell him something, he was actually on his belly creeping up behind me to see what I was looking at. Like a human snake. I didn’t know beforehand of his fear of heights and laughed before helping him draw back to safety. I’ve learned since.
Here are excerpts from Steve Graff’s story, “Inside Fear and its Disorders,” Penn Medicine News blog [paraphrased for brevity]:
Steve Graff went parasailing and panicked about 800 feet in the air. He started convulsing, vomiting, his head slouching. He writes, “Until that point, my parasailing partner stayed perfectly calm, basking in the excitement of floating above the ocean. I feared for my life. But for him, it was a rush.”
Our brains react to and process fearful situations differently. In a way, when it comes to these moments, we all start out the same, but depending on which part of our brain “wins” out, we can end up in different places. It’s also important to know that a lot of the same neural circuitry associated with our fight-or-flight response is also involved in how we experience pleasure and positive emotional states. —Steve Graff, Penn Medicine News
Some Process Fear Better Than Others
In earlier posts, I described how the fight-or-flight response sends signals from the brain’s amygdala region to the rest of our brain and throughout our body to react. Graff quotes Thea Gallagher, clinic director, Penn’s Center for the Treatment and Study of Anxiety:
“‘Riding a roller coaster can be debilitating to one person but not to another. So, it’s the same symptoms and experiences, but for some people it’s just not pleasurable. And that comes down to attribution.’”
What Gallagher is saying is one part of the brain (amygdala) is freaking out on the roller coaster, while the reasoning brain (hippocampus and prefrontal cortex) put the fear in context, using thoughts to reason with emotional

Photo: Jurassic World VelociCoaster, Universal Orlando Resort
reactions: “You’ve ridden this roller coaster 10 times already and everything turned out OK.” Graff returns to his own personal hell flying above the choppy ocean:
Up in my seat and harness high above the water, my brain seemed to convince the rest of me that the harness wasn’t enough, and I may fall, while my parasailing partner’s brain did a better job of keeping the peace. He overcame the fight-or-flight response. In fact, with all that adrenaline pumping through him, he was able to enjoy the ride. —Steve Graff, Penn Medicine News
People are attracted to the thrill experienced going through a haunted house or watching scary movies, Graff said. “There’s fear, but deep down they know there’s no real threat.”
Zoologist Mahak Jalan, Mumbai University, India, ScienceABC, shares her insight from meeting with pilots with acrophobia:
I realized that since these phobias have been learned, they can also be unlearned. This task is carried out by trained professionals who can help the brain overcome an outdated fear, or tone down the brain’s response to it. It also shows that our brain has the power to overcome its fears, and further supports the claim that these phobias can be altered, masked or “treated” if they are getting in the way of living a normal life. —Zoologist Mahak Jalan, ScienceABC
Agoraphobia
Photo: “What is Agoraphobia?” Andalou Medical Center
The most incapacitating of phobias is no longer classified as a phobia. Agoraphobia is now in a class by itself—a severe anxiety disorder that shares many symptoms with phobias and panic disorders.
By now, agoraphobia has entered the popular culture as the “shut-in,” too fearful to leave the house. The term itself is ancient Greek for fear (phobos) of the marketplace (agora). The term was first coined in 1871 by German neurologist Karl Friedrich Otto Westphal to describe a specific condition experienced by his patients as a “fear of large open spaces.”
The reality of agoraphobia is more complex and more troubling. A person with the disorder experiences intense fear of being overwhelmed, trapped (outdoors or in), helpless, or abandoned.
They sense escape is impossible or help unavailable if a panic attack or some other incapacitating reaction (to their shame or embarrassment) suddenly comes on.
In severe cases, it’s particularly disruptive. Everyday tasks — grocery shopping, riding a bus, standing in line, crowds, fear of discrimination, or even seeing a therapist — can make leaving the safety of home not worth the risk. In fact, many with agoraphobia can leave their homes, but do so with significant distress or require a trusted companion.
Common Misperceptions

Prince Harry, Duke of Sussex, younger son of King Charles III and Diana, Princess of Wales
In his memoir Spare, Prince Harry revealed he was an “agoraphobe. Which was nearly impossible given my public role,” As reported in NBC News, Harry recalled “one speech, which couldn’t be avoided or canceled, and during which I’d nearly fainted” and writes that Prince William came backstage afterwards laughing at him for being “drenched.”
Prince Harry writes,“Him of all people. He’d been present for my very first panic attack. With Kate. We were driving out to a polo match in Gloucestershire, in their Range Rover. I was in the back and Willy peered at me in the rearview. He saw me sweating, red-faced. ‘You all right, Harold?’ No, I wasn’t. It was a trip of several hours and every few miles I wanted to ask him to pull over so I could jump out and try to catch my breath.” [Article in Spare, as reported by NBC News]
In part, because of how celebrity media and TV shows portray agoraphobia, those with the disorder are often stigmatized as overly dramatic, home-bound eccentrics, who exaggerate or even fake their symptoms to call attention to themselves or get out of responsibility. In reality, most people realize their fears are irrational but still can’t overcome them on their own. This leads to social isolation, shame, and the kind of mental suffering that Prince Harry and others describe.
Another misperception, even among psychiatric professionals, is seeing agoraphobia as a panic disorder. While the two often co-occur, the recent declassification in DSM-5 reflects new understanding that agoraphobia exists without a history of panic attacks in a significant number of people. Like many anxiety disorders, agoraphobia is often misdiagnosed, which means treatments that actually can help are either delayed or never received.
Reasons for Reclassification
Agoraphobia is no longer grouped with phobias in DSM-5 because research indicates it’s a distinct anxiety disorder with different underlying causes and symptoms. It’s now attached to a broader category of anxiety disorders, alongside other distinct, but related conditions of specific phobia and social anxiety disorder (SAD). Reasons:
- A formal diagnosis requires fear or anxiety in at least two distinct situations (taking a train, walking across a park, riding an elevator, encountering a snake). This contrasts with specific phobias that center on only one specific situation. Agoraphobia’s core fear is not feeling safe or potentially losing control, rather than the presence of something disturbing.
- In previous DSM editions, agoraphobia was called a secondary consequence of panic disorder: specifically, panic disorder with agoraphobia. DSM-5 separated it out after large-scale community studies found a significant number of individuals meet agoraphobia criteria without a history of panic attacks.
- Agoraphobia is more treatment resistant to evidence-based methods like systematic desensitization (gradually reduce fear/anxiety responses to a phobia through relaxation rather than panic), which is highly effective for specific phobias.
Causes and Risk Factors
As with the majority of mental health conditions, exact causes elude the specialists. That’s because there’s probably an interplay of genes, biology, personality, and traumatic experiences that culminate in this relatively rate, but debilitating disorder. Areas of research are looking at:
- Unhappy or traumatic childhoods
- Genetic predisposition (it’s known to run in families)
- Parental overprotectiveness
- Childhood fears or night terrors
- Grief or bereavement early in life

Pablo Picasso, Guernica,1937, Museo Reina Sofía, Madrid. Picasso’s famous mural-sized painting of the Spanish Civil War shows the traumatizing effect of terrible events.
For many, agoraphobia can be traced to the trauma of major life stressors, like abuse or violent crime, car crash, death, or loss. But just as likely it’s from having a panic attack in public. Fear of another attack causes the individual to avoid the place or similar situations where it might happen again, eventually making them afraid of all public spaces.
One risk factor is a history of other mental illnesses, such as depression, other anxiety disorders (like separation anxiety), or post-traumatic stress disorder (PTSD).
Another is a person’s temperament, like a predisposition, such as a particularly anxious or nervous personality.
Biological risk factors can be an imbalance in brain chemicals like serotonin and norepinephrine, which help regulate mood and anxiety. According to research, different brain regions and brain networks that control the fight-or-flight response (FFR) can play a role. Another predisposition is alcohol or drug misuse, which can exacerbate anxiety.
Agoraphobia Prevalence
Because agoraphobia was recently reclassified in DSM-5, prevalence data is somewhat less conclusive, but the independent diagnosis has helped identify cases that previously might have gone undiagnosed or misattributed, providing a clearer picture of its actual prevalence and impact. It remains a relatively uncommon anxiety disorder in the general population, with an estimated lifetime prevalence of about 1.3%–2.6% in the U.S. and similar rates globally:
- In the U.S., .8% –1 .7% of adults have agoraphobia in a given year.
- Over a lifetime in the U.S., this is about 1.3% of adults and 2.4% of adolescents. Globally, this is around 1.2%.
- Highest rates are in the 13–17 age range (though it can begin in childhood) — but usually before age 35 (median age of onset around 20). Older adults can still become agoraphobic.
- Is diagnosed about 2–4 times more often in women than men.
- Mostly first appears after 1–2 panic attacks.
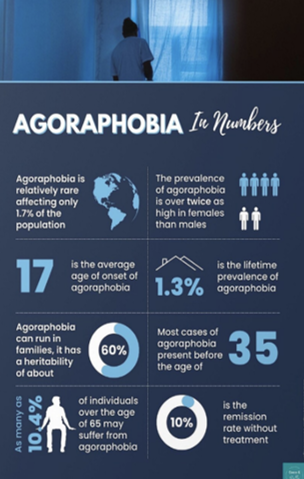
Graphic: Coco and Bella Creative
Impact and Comorbidity
Despite relatively low prevalence compared to other anxiety disorders (specific phobia affects 14% of U.S. population), agoraphobia is often comorbid with other mental health conditions and associated with more severe impairment:
- Among U.S. adults with agoraphobia, 40.6% have severe impairment.
- About 30%–50% of those with agoraphobia also have panic disorder.
- There’s substantial neurobiological overlap and comorbidity between agoraphobia and panic disorder: 50% with agoraphobia also have panic disorder. In clinical samples, as many as 95% have the combined syndrome, though
- Agoraphobia is strongly associated with dysphoric mood (major depressive disorder), as well as post-traumatic stress disorder (PTSD), social phobia (SAD subtype), and generalized anxiety disorder (GAD).
- Without professional help, full remission rates for agoraphobia are low, around 10%.
Recent Agoraphobia Research
Breakthrough research in agoraphobia are in two areas: uses of self-guided technologies and new insights into agoraphobia’s neural underpinnings, leading to refined diagnoses, successful treatments, and targeted interventions that identify brain mechanisms that predict fear and secure safety. These research breakthroughs were facilitated by the DSM-5 reclassification and updated diagnostic criteria.
Personalized Digital Treatment and Intervention innovations

Graphic: Coco and Bella Creative
Virtual reality (VR) research continues to refine hardware and software to use of personalized VR environments to simulate real-world situations, which can help people with panic and agoraphobia manage their anxiety in a controlled setting.
Smartphone-based therapy studies are evaluating the effectiveness of smartphone apps that provide self-management tools — primarily cognitive behavioral therapy (CBT) and exposure therapy — as standalone interventions. They’re designed to provide self-guided or therapist-assisted treatment, often focusing on confronting feared situations in real-life (in vivo) or virtual reality environments.
The apps incorporate psychoeducation, so people can understand their agoraphobia, the physiological symptoms of panic, and the principles of CBT. But the core element is exposure therapy to move through structured exercises to gradually face one’s fears.
Other evidence-based treatments include:
- Symptom provocation (interoceptive exposure) are exercises that actually trigger physical sensations associated with panic (a pounding heart) to help users realize these symptoms are uncomfortable but not harmful (not having a heart attack).
- Anxiety journaling and tracking of panic attacks, avoidance behaviors, and anxiety levels to identify patterns and monitor progress.
- Coping strategies taught by the apps, like breathing techniques, relaxation exercises, cognitive restructuring (changing unhelpful thoughts), and self-soothing strategies.
- Goal setting for recovery journey, such as spending a certain amount of time outside their home or visiting a specific place.
- Therapist integration on apps designed for a blended-care approach, allowing users to share their tracked data and progress with their therapist for guidance and support.
Studies show agoraphobia-specific smartphone apps are more effective in reducing symptoms and controlling anxiety than general stress-reduction apps, particularly for the homebound. But, as research finds, the most effective way to achieve full symptom remission is by combining therapies: cognitive behavioral therapy (CBT), medication, and digital integration.
Understanding Neural Mechanisms
Neuroscience research has found altered brain function, neural circuits, and neurochemical pathways involved in regulating fear and anxiety during active agoraphobic and panic attacks. Neuroimaging studies not only show this, but also show brain alterations when “agoraphobic stimuli” (crowds, elevators) are anticipated.
Photo: National Institute of Mental Health
The amygdala, prefrontal cortex (PFC), and hippocampus are some of the brain regions involved in anxiety and fear. The neural mechanisms involved in agoraphobia show dysfunction in these areas and in the neurocircuitry that connects them. There’s an imbalance between areas that detect threats and those that regulate emotional responses and return to safety. The brain and the science are too complicated for me to adequately cover. For the dedicated, however, here’s how a team of Dutch researchers describe brain chain reactions that respond differently in the case of “pathologic anxiety”:
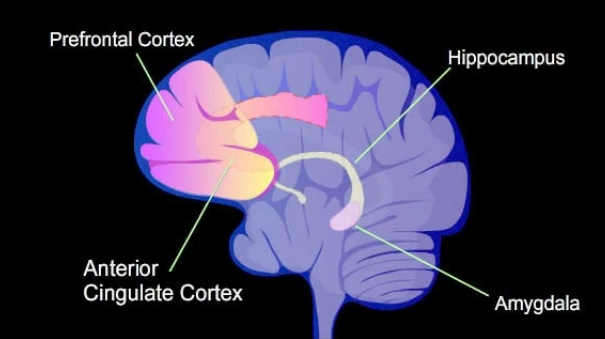
The amygdala serves as a central hub in the fear detection and response network, mediating immediate threat responses, while the bed nucleus of the stria terminalis is implicated in sustained anxiety and risk assessment. The ventromedial prefrontal cortex exerts inhibitory top-down control over amygdala activity and fear responses, and dysfunctions in this control mechanism are associated with pathologic anxiety.
Increased activity in the insular cortex during anticipation of agoraphobic stimuli correlates with symptom severity. Altered hippocampal activity has also been observed in agoraphobia. The locus coeruleus and periaqueductal gray are components of the fear detection and response network implicated in panic disorder and agoraphobia. —Brenda Penninx, et al., Vrije Universiteit Amsterdam, Netherlands, “Agoraphobia,” Science Direct
Anticipating agoraphobic stimuli (fear of another panic attack) shows increased activity in the brain’s insular cortex, which helps process internal bodily sensations (interoception). Dysregulation of the brain’s interpretation of these interoceptive signals is significant and a reason why fear and anxiety are so intense and persistent.
Other research, in brief
Overall, recent studies emphasize the complexity of agoraphobia’s neurobiological basis, moving beyond a simple “fear of fear” to involve specific dysfunctions in how the brain processes sensory input, manages threat responses, and regulates emotion. These findings are paving the way for more targeted and personalized therapeutic approaches. —Brenda Penninx, et al., “Agoraphobia,” Science Direct

Sources: Science Direct, Chat GPT, Wikipedia
Evolutionary Psychology: Primary and Secondary Agoraphobia
According to, evolutionary psychology views the more unusual primary agoraphobia without panic attacks as due to a different mechanism from agoraphobia with panic attacks.
- Primary agoraphobia without panic attacks may be a specific phobia that had an evolutionary advantage for our forebears, so they avoided exposed, large, open spaces without cover or concealment.
- Secondary agoraphobia with panic attacks may be a secondary avoidance response to panic attacks, due to fear of the situations in which the panic attacks occurred.
Later posts discuss diagnoses, symptoms, and treatments for agoraphobia.
Neuroscience research has found altered brain function, neural circuits, and neurochemical pathways involved in regulating fear and anxiety during active agoraphobic and panic attacks. Neuroimaging studies not only show this, but also show brain alterations when “agoraphobic stimuli” (crowds, elevators) are anticipated.
Coming Up Next

Phobias can result in anxiety or panic attacks, and multiple panic attacks can be diagnosed as a panic disorder. All these conditions carry disturbing, disruptive, and demoralizing psychological and physical symptoms. This includes fear of fear. That’s the basis of agoraphobia, covered in this post, and we’ll see it in Post 11: Anxiety Attacks vs Panic Attacks vs Panic Disorder.
Sources