On Anxiety and Panic Disorders
Show Table of Contents
INTRO
1. On Neurodivergence and Otherness: An Introduction
SENSES AND SENSORY SENSITIVITIES
2. Senses Count
3. Neurobiology for Dummies
4. Sensory Transmission and our Reward System
5. Sensory Receptors are the Body’s Cellular Plan
6. A Synthesis: Sensory Systems and our Emotions—Part I
7. A Synthesis: Sensory Systems and our Emotions—Part II
8. Sensory Disorders and Sensitivities
9. Etan’s Story
10. Synesthesia: Difference, But Not Disorder
11. Synesthesia, Creativity, Artistry—Part I
12. Synesthesia, Creativity, Artistry—Part II
AUTISM AND THE NEURODIVERSITY MOVEMENT
13. From “Mental Defectives” to Autism Spectrum Disorder
14. Changing Conception of Autism
15. Autism Diagnoses and Behavior Patterns
16. Autism Treatments that Help
17. Early Start Autism Treatment: A Case Study
18. Neurodivergence and the Neurodiversity Movement
19. Neurodiversity Takes Flight
ADHD
20. ADHD and Neurodevelopmental Disorders
21. ADHD: A Preponderance of Risk Factors and Symptoms
22. ADHD: Inattentive, Impulsive…and Hyperactive?
23. ADHD: Named, Renamed, Still Needs a New Name
24. ADHD: Treatment and Coping Skills for All Ages
LGBTQ+
25. Neurodiversity and the LGBTQ+ Fight
26. LGBTQ+ Identity and Expression
27. LGBTQ+ and Mental and Behavioral Healthcare
ON LANGUAGE
28. Language Matters In and Around Neurodiversity
29. Neurodivergent Language Difficulties
30. Disability-Inclusive Language Guidelines
ON CREATIVITY AND GIFTEDNESS
31. Neurodiversity and Creativity
32. Giftedness is a Piece of Neurodivergence
SELF-IDENTITY
33. Self-Identity: The Cornerstone of Neurodiversity
34. Early Theories of Self-Identity Formation
35. Contemporary Theories of Self-Identity Formation
36. Authenticity and the Search for Self
37. Self-Schemas and Neurodivergence
38. Self-Labeling and Parts Work
39. Cognitive Complexity and Empathy
IMPROVING LIFE FOR NEURODIVERGENT PEOPLE
40. Reducing Neurotypical-on-Neuroatypical Conflict, Part I
41. Reducing Neurotypical-on-Neuroatypical Conflict, Part II
42. Communicating Across the Neurospectrum, Part I
43. Communicating Across the Neurospectrum, Part II
44. Neurodiversity: Advocacy, Education, and Lifestyle
45. Neurodiversity and Work
IN CONCLUSION
46. In Conclusion: Neurodivergence and Inspiration
1. On Anxiety and Panic Disorders: An Introduction

In writing about mental health issues, I see the most common, basic AND complex of psychiatric disorders to be anxiety. Well, who doesn’t experience anxiety from time to time? I have an anxiety disorder. It could be situational, as I’m worried about my sons, my retirement finances, lot of things — but that’s not owning it. I have an anxiety disorder, not just a series of worries.
This series is as much about self-scrutiny as it is about reporting on the mental disorders of others. I’ve suffered from anxiety, with insomnia, tension headaches, knotted gut, My sons have anxiety disorders, expressed in extremely different ways.
Anxiety is a deeply foundational emotion—in fact, the wellspring of so many other mental health conditions that we’re simply unaware of the power and persistence of anxiety in our lives. In the give and take that’s life, we need to protect our nervous systems from the beginning of the path (point of stimulus) to its mix with cognition (in the brain) to its final destination (muscles/glands), so we move, react, act. Some of it voluntary and a lot involuntary. We nourish our brains through intellectual and artistic pursuits, building relationships, seeking our community, and treating our bodies well. We hurt ourselves by masking and maladapting behaviors that interrupt our natural processes. And many of us are born with built-in obstacles to natural processes that we have to first understand before we can overcome them. I’ve experienced anxiety attacks at night, so I’ve decided to figure them out. And relatedly, explore panic attacks, which are even more debilitating and make you think you’re about to die—not to be too dramatic about it.
Transmission of Stimuli via Sensory Receptors
I decided to learn more about anxiety attacks and panic attacks, what causes them, how they’re the same and different, and what to do about preventing them (best) or reducing their severity (next best). It is impossible to explain a slice of anxiety without the whole pie. We need to understand anxiety. My focus is on severe anxiety disorders and their evolutionary and biological role in making us who we are today—and what we can do about reducing pain and heightening joy.
Also, brain structure, brain chemistry, and neurotransmitters. I love neuroscience—even if I can’t understand most of what I read. Take this:
Every time I look something up, I have another three things to look up. I might have given up if I wasn’t so dedicated to pushing the limitations of my brain function to understand brain function (probably an anxiety-riddled compulsion). I’ll judiciously share what I learn, because if anxiety is foundational to understanding our mental health, then brain function is foundational to understanding anxiety. This series covers generalized anxiety disorder (GAD), social anxiety disorder (SAD), anxiety attacks, panic attacks, phobic disorders, and agoraphobia. My focus is on those of us who have suffered from an anxiety or panic attack away from home — and are living a different life because of it.
The Greatest Impact on Human Behavior: Pure Emotion

Vasily Kandinsky, Color Study. Squares with Concentric Circles, 1913, Städtische Galerie im Lenbachhaus, Munich
Social science has defined the building-block emotions that make us human. Since the 1960s, primary and secondary emotions have grown from Eckman’s six to combinations of up to 30. Research suggests we’ve evolved from cave dwellers with a set of emotions that were key to our survival and propagation. It’s theoretical, of course, but what a way to be grounded in our essential selves—and humbled by our inheritances that go far back, beyond mom and dad.
In this post, I’ll compare primary and secondary emotions to basic psychological states that push us along the anxiety spectrum—from normal to less normal to neuroatypical to someone hiding in their house terrified of what awaits them on the other side of the door. Questions to explore:
- What’s the relationship between fear (primary) and anxiety (secondary)?
- What causes emotions to wreak havoc on our bodily systems?
- What does emotional health look like?
- Is understanding the impact of our emotions on our behavior helpful to our wellbeing?
Emotional Building Blocks
Peripheral nervous system
“Primary emotions are often very strong, which makes them easy to identify. They are thought to be instinctive, primal, and sensitive,” writes Olivia Guy-Evans, Simple Psychology. Primary emotions, she continues, are pre-cognitive and adaptive. They cause us to react instinctually and immediately, without cognitive interruption, to ensure our safety in a dangerous world.
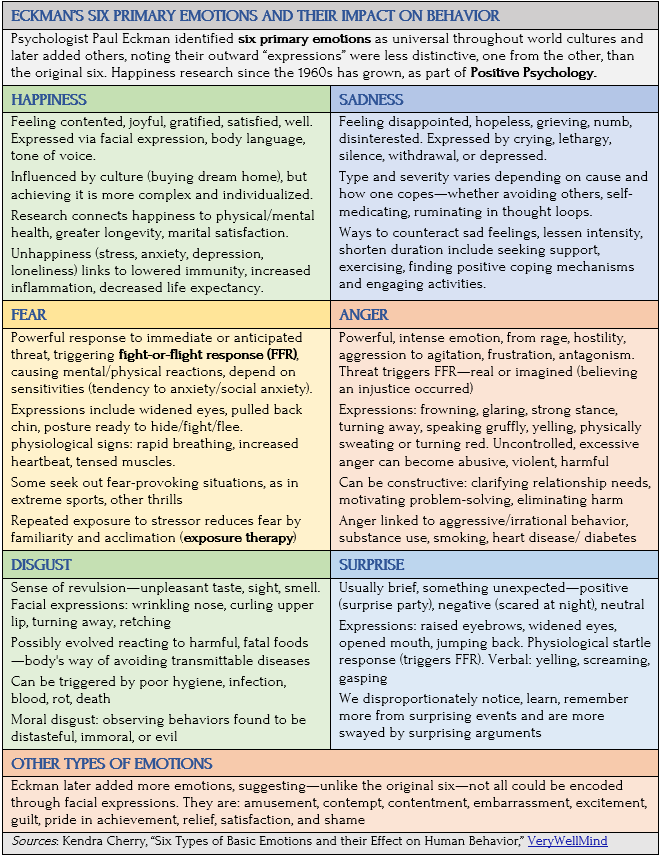
Beginning in the 1970s, Paul Ekman, renowned psychologist and professor emeritus at the University of California, San Francisco, was a pioneer on researching primary emotions and their facial expressions. With Wallace Friesen, he developed the Facial Action Coding System (FACS) to describe all visually discernible human facial movements.
FACS breaks down emotions into “action units” (AUs), identifying and assigning a code to specific facial muscle movements. AU6 is the “cheek raiser” (crow’s feet around the eyes) and AU12 is the “lip corner puller,” better known as a smile. FACS was used by researchers to study emotions, by animators to create realistic facial expressions, and computer scientists for facial recognition tasks. Ekman even consulted with Hollywood for his work on microexpressions and detecting deception.
Here’s a chart on Eckman’s groundbreaking research that was able to, for the first time, define and categorized highly distinctive emotions—easily recognized by facial expression, body language, and physical responses.
Emotional Intensity in Combination
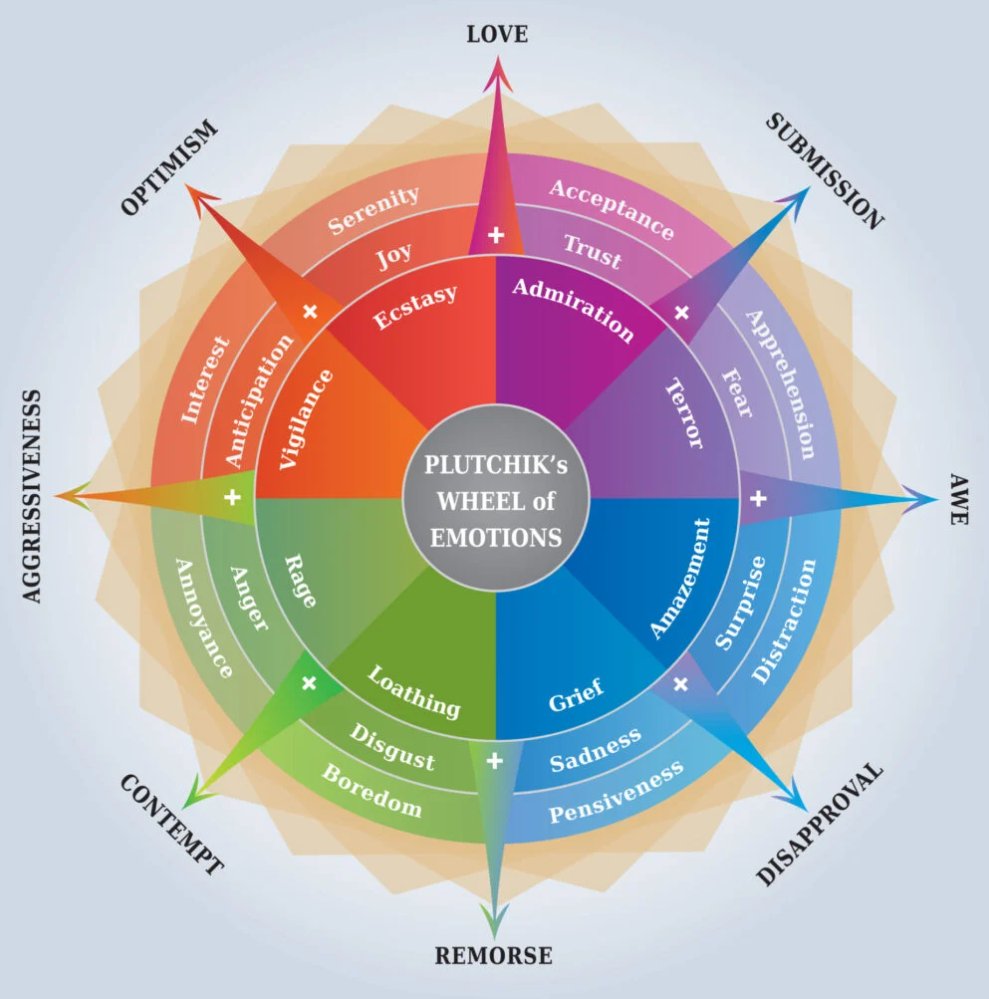
Psychologist Robert Plutchik developed wheels of eight building-block emotions—adding trust and anticipation to Ekman’s original six. In combination, these baseline emotions formed more complex and varied feelings—much like a color wheel mixes primary and secondary colors to create endless shades and tones. As red and yellow create orange, joy and trust create love.
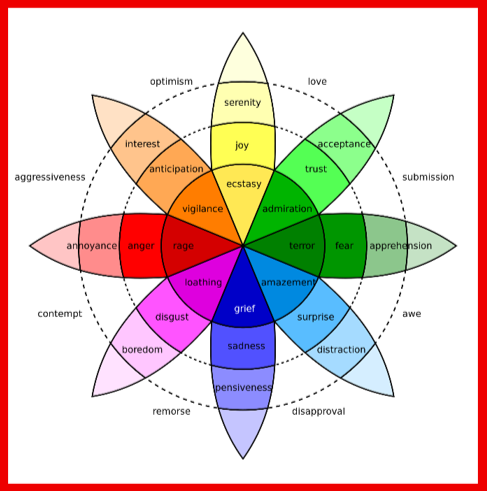
Robert Plutchik’s emotion intensity wheel. Source: Simon Whitely

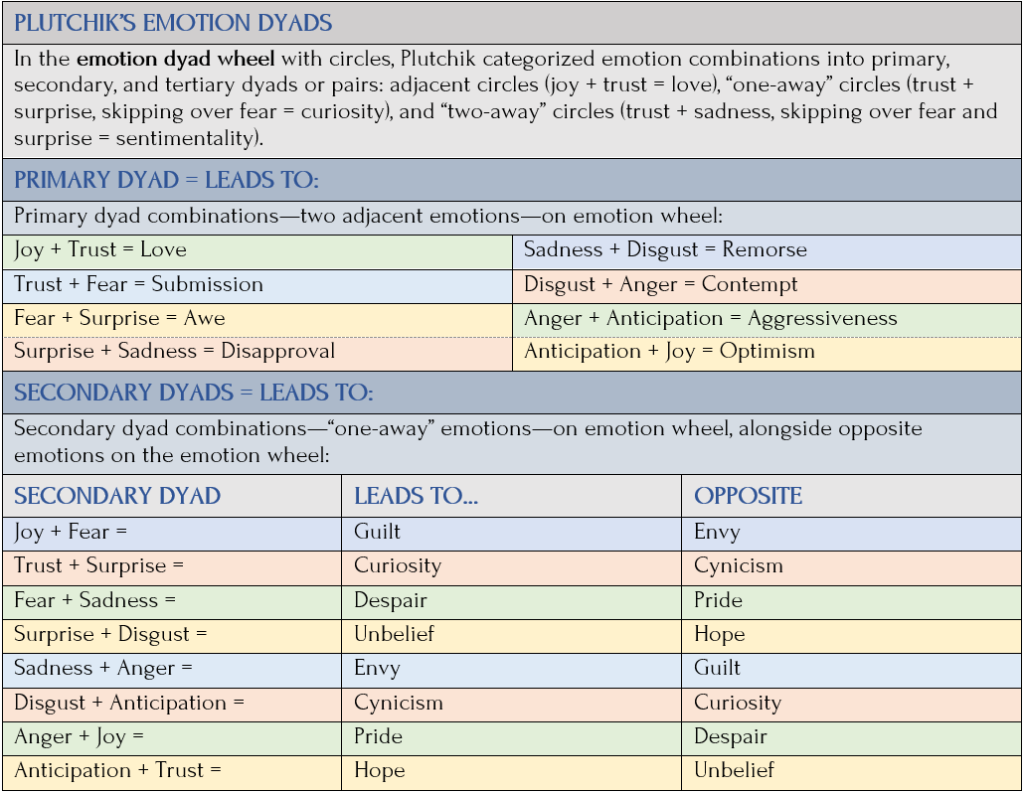
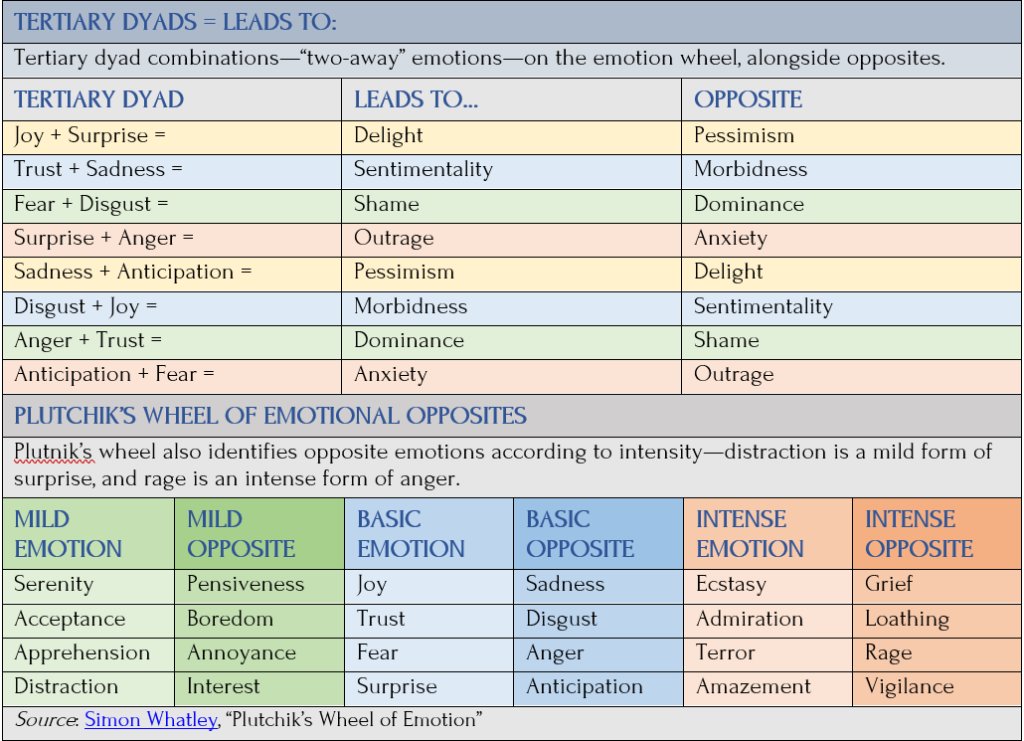
Robert Plutchik’s emotion dyad wheel. Source: Simon Whitely
In Plutchik’s “petal” emotion intensity wheel, basic emotions intensify toward the center or become milder toward the tip of the petal. Joy is serenity at its least intense and ecstasy at its most. If left unchecked, intense negative emotions can become destructive or lead to anxiety and depression. In his emotion dyad wheel with circles:
More recent theories and research classified different types of emotions. According to VeryWellMind, a 2017 study identified 27 different categories of emotion—less distinctly unique than the original six and experienced more along a gradient.
Next-Level Secondary Emotions
Emotions Wheel, Simple Psychology
If primary emotions are immediate, instinctual, and sensitive responses to stimuli, then “secondary” emotions are reactions to primary emotions. They’re more complex, influenced by personal experiences, beliefs, and thoughts, writes Guy-Evans. I paraphrase:
Secondary emotions are felt after experiencing a primary emotion. Rather than instinctual, they are often habitual or learned responses. They influence our behavior, increase the intensity of our reactions, and last longer than primary emotions, as in these examples:
- After feeling anger (primary), we may feel shame (secondary), because we had time to consider our angry outburst and not be so happy about it.
- After feeling joy (primary), we may feel pride (secondary), because we take credit for the experience.
- After feeling fear (primary), we may feel anxiety (secondary), because now we realize what a close call it was and are worried about it happening again.
Less sensitive secondary emotions provide cover for more sensitive primary emotions as a way of protecting the self from being vulnerable. Yet, they can lead to more hurt and pain as they accumulate, especially if they are emotions like guilt, shame, jealousy, envy, resentment, frustration, and remorse. These emotions are often learned in childhood.
Healthy Emotion vs Unhealthy Emotional Stress

Photo: Vecteesy
A precarious ridge divides healthy emotion and unhealthy emotional stress or mental disorders. With better awareness and understanding of what side of the ridge we descend from, we might improve how we respond to people, situations, and ourselves in our daily interactions.
Mental disorders are less dots in time or space, less discrete stars in the sky, and more comets streaking across the universe, sliding along a spectrum: from good to bad to worse. Here’re two kinds of anxiety spectra:
From healthy (adaptive) to unhealthy (affecting daily life) to debilitating (phobic fear) to life turned upside down (panic disorders, agoraphobia)
From single anxiety disorder (generalized anxiety disorder—GAD) to single comorbidity (GAD and major depressive disorder—MDD) to multiple, comorbid conditions (GAD, anxiety attacks, MDD, and trauma).
Common comorbidities with anxiety disorders include MDD, obsessive-compulsive disorder (OCD), PTSD, and substance abuse disorder (SUD)—though, there are many, many more.
Anxiety is what experts call an adaptive, affective emotion—it changes flexibly depending on the circumstance and is concerned with the experience of the feelings. Anxiety stays on the healthy side of the ridge as long as it motivates you to get to a place of physical, emotional, or psychological safety.

Glossophobia, or fear of public speaking. Photo: Leaders Speaking
- Healthy anxiety: Let’s say you have a make-or-break, public presentation and, as time grows near, you find yourself increasingly anxious. After you give a successful presentation, your mood soars with gratitude that it went well and that it’s over. This is healthy anxiety.
- Unhealthy anxiety: Now let’s say, after your talk, you wonder whether you prepared enough or whether others thought you looked unprepared. You feel no relief it’s over and, instead, fret about what will be required of you next month. If you didn’t do so great this time, next time you’ll do worse. You retreat from volunteering for challenging opportunities, and someone else takes over the public speaking role. Meanwhile, you start having stomach aches and missing work, you snap at your spouse, and you start watching excessive TV. Anxiety crossed the ridge—your exaggerated emotional response has interfered with your ability to function.
I plan to discuss what we can do for ourselves—starting with self-awareness and running through a lot of other “self-hyphenates,” like self-esteem, self-compassion, and even self-love. And what you can’t do for yourself, when you absolutely need professional intervention and guidance, if not medication, to get better.
Start by Committing to Your Health and Wellbeing
A lot of us slip off the ridge to the dark side when we don’t commit to our own health. We don’t take it seriously. If one drink is good, three is better. We’ll quit cigarettes next year. We deny a connection between our mental and physical health. We deny, suppress, or hide from what’s happening to us. We might retreat, or we might act out.
Depending on our choices, we’re moving in the right direction for future wellbeing or we’re not. Doing nothing makes it worse. In a lifetime, most of us, being human, do both. But at what cost? With how many wasted years and lost jobs and relationships?
Coming Up Next

A lot of us slip off the ridge to the dark side when we don’t commit to our own health. We don’t take it seriously. If one drink is good, three is better. We’ll quit cigarettes next year. We deny a connection between our mental and physical health. We deny, suppress, or hide from what’s happening to us. We might retreat, or we might act out.
Depending on our choices, we’re moving in the right direction for future wellbeing or we’re not. Doing nothing makes it worse. In a lifetime, most of us, being human, do both. But at what cost? With how many wasted years and lost jobs and relationships?
Sources
{kind=link}