On Anxiety and Panic Disorders
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
2. Emotional Health vs Mental Health

From understanding the distinct features of building-block emotions, we can gain a picture of emotional health. In this post, I’ll probe how emotional health is both sharply different from — and interdependent with — mental (or psychological) health.
Hopefully, knowing this can lead us to finding better ways to approach our issues and experiences.
We’re in a better position to recognize when healthy crosses over to unhealthy — and when it’s time to stop the downward spiral and get some professional help.
Unless otherwise specified, sources for this post are psychiatrist Richard Crabbe’s article, Free by the Sea, and PubMed/NIH research papers.
Emotional Health

Photo: Freerange Stock
Emotional health is concerned with our emotional states — our happiness or satisfaction in life. It’s the result of how effectively — how positively — we deal with frustration, anger, sadness, or even joy. We are emotionally healthy when we have emotional awareness and understanding of our emotions and those of others.
Emotional health is linked to mental (or psychological) and physical wellbeing. Being able to manage our emotional reactions to life’s stressors in a positive, calm way can help us avoid anxiety’s debilitating effects. This is called emotional regulation — or affect regulation — defined by the National Institute of Health (NIH) as the ability to manage one’s own emotional responses [paraphrased]:
Emotional regulation is the ability “to increase, maintain, or decrease the intensity, duration, and trajectory of positive and negative emotions.” Positive emotional regulation allows flexibility in emotionally taxing situations and leads to better outcomes in relationships, at work, or in school — and it increases overall happiness.
The flip side is also true. When we don’t work through uncomfortable emotions or stressful situations in a positive way and instead try to suppress, ignore, or defend what we’re feeling — or escape with risky behaviors — unchecked emotions can worsen symptoms and overall health.
Body chemistry, unchecked emotions, and unhealthy habits combine to damage our mental and physical health — leading to anxiety, depression, headaches, stomachaches, insomnia, addiction. Smoking, drinking, or overeating to relieve stress raises the risk for cancer, heart disease, diabetes, obesity, and other illnesses.
Emotions are not just “feelings” or mental states, but are accompanied by physiological and behavioral changes that are an integral part of them. —Swiss clinical psychopharmacologist Thierry Steimer, “The biology of fear- and anxiety-related behaviors,” PubMed
Emotions are experienced or expressed at three interrelated levels:
- Mental or psychological level (states of mind)
- Neurophysiological level (states of brain activity)
- Behavioral level (ways of acting or conducting ourselves, especially to others)
These three complementary aspects are present in even the most basic emotions, such as fear.
Mental Health
Mental health digs deeper into the brain-mind-body connection than emotional health. It affects our cognitive (thinking), behavioral (acting), and neurochemical (brain) functioning, as in psychological or neurological conditions.
This is not to say emotional health is less important. Mental health strongly involves emotional health. It’s less about how well we handle difficult emotions and more about how we think and feel about ourselves — and how these thoughts and feelings influence our behavior.
Mental health embraces many ways of being, stemming from the inheritable (genetics, brain chemistry) to the environmental (how we were raised, existence of trauma, extreme poverty, or global worries, like climate change, war, pandemics) to the situational (what we’re going through today, difficulties at school or work, in relationships).
Unhealthy mental habits can lead to emotional distress. Untreated mental health disorders have a powerful impact on physical health.
The phrase “mental health” covers a vast range of topics from anxiety disorders to autism spectrum disorder, while “emotional health” is more subjective in nature — it’s all about how one feels emotionally. It’s important to remember that emotional health does not necessarily imply mental health, although having good emotional wellbeing is certainly beneficial for overall mental wellbeing, too. —Richard Crabbe, Free by the Sea
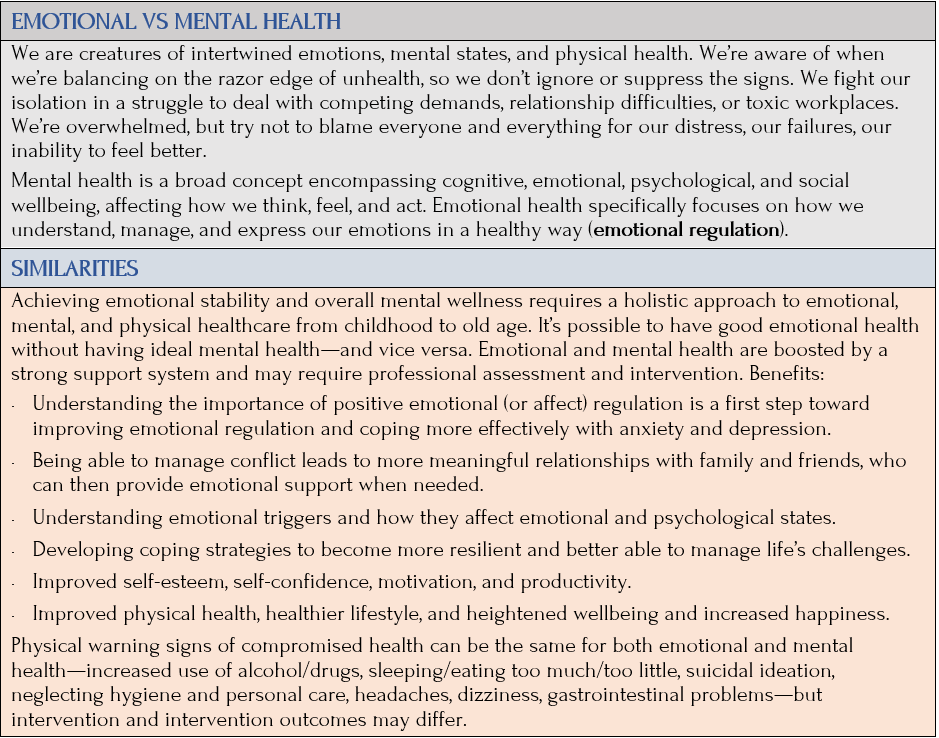
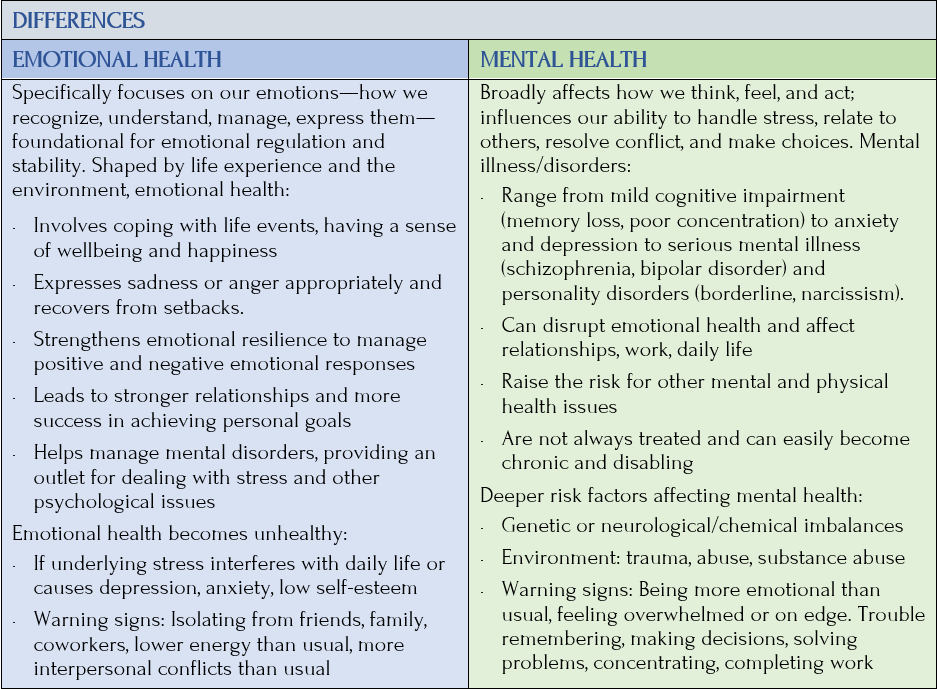
Emotional vs Mental Health
The next two charts show the similarities and differences in emotional vs mental health
Core Mental Health States
- Fear is a primary emotion. Adaptable, affective, pre-cognitive.
- Anxiety is a secondary emotion — mixing fear with anger, jealousy, hurt, or sadness. Adaptable, affective AND cognitive.
- Anxiety disorder is a basic, but serious mental disorder — a chronic, uncontrollable anxiety that causes significant life problems.
Fearing Our Fears
In his Psychology Today article, “The (Only) 5 Fears We All Share: When we know where they really come from, we can start to control them,” author/thinker Karl Albrecht cites President Franklin Roosevelt’s famous quote, “The only thing we have to fear, is fear itself.” Albrecht creates a classification of fear categories that show how we fear our fear.
That strange idea of “fearing our fears” becomes less strange when we realize that many of our avoidance reactions — turning down an invitation to a party if we tend to be uncomfortable in groups; putting off a doctor’s appointment; or not asking for a raise — are instant reflexes that are reactions to the memories of fear. They happen so quickly that we don’t actually experience the full effect of the fear. We experience a “micro-fear” — a reaction that’s a shorthand code for the real fear. This reflex reaction has the same effect of causing us to evade and avoid as the real fear. This is why it’s fairly accurate to say that many of our so-called fear reactions are actually the fears of fears. —Karl Albrecht, Psychology Today
By understanding and gaining information from and about our fears, Albrecht says, “we can think about them consciously. And the more clearly and calmly we can articulate the origins of the fear, the less our fears will frighten us and control us.”
Albrecht’s five fear categories are thought-provoking and reach beyond us, extending to society itself. His categories incorporate phobic fears and illuminate the universality of our fears.
Karl Albrecht’s Feararchy
Albrecht’s “Feararchy” and what he included in each “fear of” category [paraphrased for brevity]:
Extinction: Fear of annihilation, of ceasing to exist, arousing a primary existential anxiety in all of us. Fear of heights gives a panicky feeling as we imagine falling from the cliff.
Mutilation: Fear of losing any part of our body, having our body’s boundaries invaded, or of losing the integrity of any part or function of our body. Includes animal phobias.
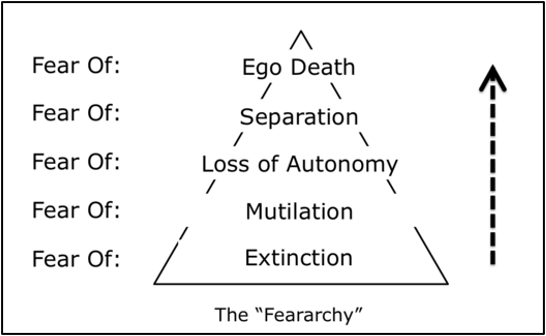
Source: Karl Albrecht, “The Feararchy,” 2007
Loss of Autonomy: Fear of being immobilized, paralyzed, restricted, entrapped, imprisoned, smothered, or otherwise controlled by circumstances beyond our control, including claustrophobia and fears of intimacy and commitment. Anger covers up the fear of losing autonomy; also “Those who make us fearful will also make us angry.” Destruction of a culture or a religion by an invading occupier represents a collective fear of losing autonomy.
Egon Schiele, Portrait of Albert Paris von Gütersloh, 1918
Separation: Fear of abandonment, rejection, and loss of connectedness — of becoming a non-person — not wanted, respected, or valued by anyone else. Getting the “silent treatment” can devastate us, either from an individual or a group. Feelings of jealousy, embarrassment, guilt, shame, humiliation are fears of separation.
Ego-death: Fear of humiliation, shame, or other means of profound self-disapproval that threaten the loss of integrity of the self, like being devalued or no longer feeling lovable, capable, and worthy. Fears of failure or public speaking are fears of ego-death. So is feeling envy. Religious bigotry and intolerance are fears of ego-death on a cosmic level and can extend to existential anxiety.
What Albrecht is saying is fearing our fears is anxiety. I find this so profound. The core mental health states — fear, anxiety, anxiety disorder — unchecked, unexplored, misunderstood, ignored, avoided, and untreated threaten us. As individuals and as a society.
Anxiety is Normal
If it’s largely true that anxiety is the foundational springboard for all mental disorders not sprung from mood or personality disorders, then we can spend less time thinking about how much can go wrong. Simply, solving anxiety solves many other problems. Not easily, but it’s a place to start.
Exploring the evolutionary purpose of fear and anxiety might tell us why some of us are more prone to being disabled by anxiety disorders than others.
Anxiety is a normal part of human existence, experienced by most people throughout their lives. Indeed, the only individuals without anxiety are sociopaths, who are famous for their disregard of social norms. The rest of us suffer from a vulnerability to anxiety and the multiple ways that it can be used for socialization. Attempts to explain anxiety as a reasonable reaction, or valuable over-reaction, to actual physical danger do not do justice to the robustness, intensity, and resiliency of anxiety as a ubiquitous dimension of human existence. —Jeffrey J. Mermelstein, clinical psychologist, evolutionary scientist
There are two things I appreciate in Mermelstein’s quote. Only sociopaths feel no anxiety, AND anxiety is robust, intense, resilient, and ubiquitous. Sara Berg, writer for the American Medical Association NewsWire, provides another global take on anxiety/anxiety disorders:
Anxiety is a shared human experience. The prospect of speaking in front of a large group of people or taking a test can trigger anxiety. Yet this unease can also serve as a catalyst for diligent preparation and rehearsal. But if feelings of extreme fear and turmoil become overpowering and hinder routine activities, this may indicate an underlying anxiety disorder. —Sara Berg, news editor, “What doctors wish patients knew” series
Here are some questions Mermelstein and Berg raise for me:
- What are the evolutionary benefits of anxiety? Are they the same in modern times?
- Did fear come first or did fear and anxiety arrive at the same time?
- What role does the fight-or-flight response (FFR) play in human development?
- How does anxiety disrupt the normal brain-mind-body connection?
- How is anxiety used for socialization?
- When does anxiety turn into anxiety disorder?
I’ll return to these authors in future posts. First, some global facts and statistics.
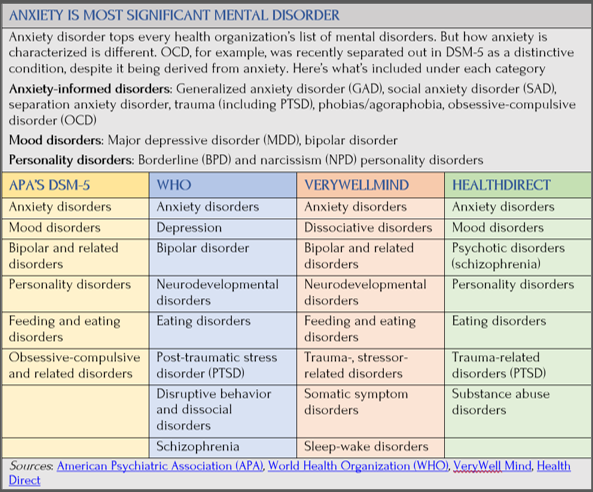
Anxiety Tops the List of Mental Disorders
According to the Centers for Disease Control and Prevention (CDC), there are more than 200 types of mental illness. The American Psychiatric Association’s DSM-5 includes more than 450 definitions of mental disorders. A Google search shows how a diverse set of mental health organizations categorizes mental, behavioral, and personality disorders. They are quite different except in one respect: they all place anxiety disorders as the most common and prioritized of conditions:
Prevalence of Anxiety Disorders in the World Population
Anxiety disorders (GAD, panic disorder, agoraphobia) are the most common U.S. mental health concerns, affecting 20% of all adults — or 40 million adults — within a given year.
- Lifetime rates are even higher and affect more women (40%) than men (26%), especially during midlife
- During pregnancy and postpartum, GAD affects close to 11%
- Typically begins in childhood and early adulthood, and symptoms appear to decline with age
- The U.S. Preventive Services Task Force (USPSTF) recommends physicians screen for anxiety disorders in all adults up to 65 and all woman who have just given birth (JAMA)
Source: National Institute of Mental Health (NIMH)
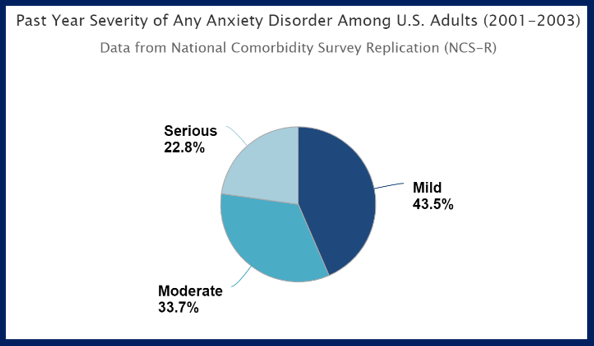
Among those with anxiety disorders, 3/5 have a moderate-to-serious disorder (chart includes panic disorder, GAD, phobias, PTSD, OCD, and separation anxiety disorder)
The National Institute of Mental Health (NIMH) reports anxiety disorders vary by age.
In adults:
- 22% are ages 18–29
- 23% are ages 30–44
- Drops to almost 21% for those ages 45–59
- Affects only 9% of people ages 60+
Experience of GAD by onset age:
- Childhood or adolescence, with most before age 21
- About 7% of children (ages 3-17) each year
Experience of GAD compared with other racial and Hispanic-origin groups:
- Non-Hispanic white adults: most likely
- Non-Hispanic Asian adults: least likely
According to WHO, anxiety disorders are the world’s most common mental disorders — a major global burden of disease.
These disorders are associated with a considerable degree of impairment, high health-care utilization, and an enormous economic burden for society. Although effective psychological and pharmacological treatments exist for anxiety disorders, many affected individuals do not contact health services for treatment, and of those who utilize these services, a high percentage is not diagnosed correctly or not offered state-of-the-art treatment. —American Medical Association NewsWire podcast
WHO’s large-scale population surveys in 2019 estimated:
- Anxiety affected 4% of the global population, translating to 301 million people
- Up to 34% of the population are affected by an anxiety disorder during their lifetime
- Some types more prevalent than others; GAD severity differed by sociodemographic
- About 1 in 6 or 16% adults (ages 18+) experienced anxiety in prior 2 weeks of survey. Symptoms were mild (9.5%), moderate (3.4%), or severe (2.7%)
- More women are affected than men
American Medical Association NewsWire podcast:
- 1/3 of Americans have anxiety during their lifetimes, with 25% of those diagnosed with an anxiety disorder
- Age of onset: Social anxiety disorder (SAD) — ages 14-15. Panic disorder: usually young adulthood. GAD: usually during 30s
Treatment Statistics
No matter how severe, anxiety disorders can be treated, generally with short-term, effective, and cost-effective methods. Despite this:
- Anxiety disorders are substantially underrecognized and undertreated
- Only 1/4 people in need (27.6%) receive treatment
- Untreated anxiety disorders are chronic, but decrease naturally with older age
- Anxiety disorders are highly comorbid with other anxiety and mental disorders
- Barriers to treatment: unaware it’s a treatable condition, poor government investment in mental health, lack of trained healthcare providers, social stigma
In 2019 global survey, bullying victimization affected 7% of the world population (meaning they lost years of their life to anxiety disorders as a result of being bullied), mainly among those ages 5-9. This showed a dramatic increase in almost all countries, compared with 1990.
Survey recommendations to reduce the burden of anxiety disorders would require:
- Controlling risk factors, such as bullying
- Distributing effective mental health knowledge
- Diversifying and adapting intervention strategies to specific populations
Coming Up Next

In Post 3: Fear vs Anxiety, I’ll return to the topic of fear and anxiety and their evolutionary benefits — and what that means for 21st-century mental and emotional distress.
Sources