On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
9. Phobias and the Rapid Onset of Fear

Most of us can conjure up moments in our life when we felt extremely uneasy or anxious in certain situations or in anticipating demands on us to “perform” or meet someone’s expectation of us. And, we all have reasonable or slightly unreasonable fears, such as spiders, injections, or bumpy air flights. Usually, our feelings resolve once we escape the spider, get the vaccine, land in the airport, or hear the final applause to our talk or dance recital. We’re relieved it’s over, we survived, and in fact we might have deserved the standing ovation.
For many of us, though, fear and anxiety are overwhelming, irrational, and uncontrollable — out of proportion to any actual danger and persisting well past the feared experience ends. We feel internal threats, from unexplained body sensations, and external, from spiders, yes, but also from the scary way a stranger acted that maybe spelled danger.
Experiencing phobic fear is a type of anxiety disorder. Like in the body’s fight-or-flight response (FFR), anxiety appraises the stressor as threatening, which arouses emotional and bodily reactions of intense fear. Maybe we don’t fight or flight, but seek avoidance and safety behaviors. These are called interoceptive avoidance behaviors. Short term they do indeed calm the rising fears. But, over the long-term, they prevent new learning about the true nature of the threat and worsen mental and physical symptoms.
Misinterpreting Body Sensations
When our bodies are aroused to a state of intense, exaggerated fear, we can sense our heart rates are speeding up or we can feel breathless, clammy and sweaty, fuzzy in the brain, overheated or chilled, dizzy, lethargic, queasy, or shaky. Many of these physical symptoms can be actual medical conditions (heart disease, for example) or feel like them. But not understanding what’s actually causing our body sensations can trigger greater emotional and physical reactions and even more fear and anxiety.
According to Psychology Tools, this creates a rapidly escalating feedback loop, a vicious cycle. Physiological reactions to threat exacerbate the feared body sensations, which in turn lead to increasingly catastrophic misinterpretations, such as a panic attack.
Those suffering from a wide range of disorders — panic disorder, health anxiety (worry you’re having a heart attack), chronic pain, irritable bowel syndrome, and chronic dizziness — are more prone to this misinterpretation. Someone suffering this way naturally seeks to avoid what triggered their fear to tamp down the stress and protect themselves from the threat — or the possibility of being trapped in a creaky old house after midnight.
With a certain amount of effort, one can avoid situations that trigger fear in the external world, but it’s much harder to avoid one’s own body sensations. Misinterpretation can result in ineffective behavioral changes. Last three examples drawn from Psychology Tools:

- In Byrnne’s telling of her full-blown panic attack [post 4], she wrongly appraised her racing heart and chest pain as “I’m having a heart attack.” Prematurely grieving her husband and children, she prepared to die on her way to the hospital.
- A man in his mid-30s had sharp back pain, appraising it “as a sign of damage” and reduced his regular exercise regimen to avoid further pain. Over the next year, his lack of movement caused further physical deconditioning and more pain in movement.
- A young woman with mental illness in her family felt funny when drinking coffee to relieve fatigue. She felt she was “losing my mind” and felt terrified, subsequently avoided caffeine, and monitored her internal mental state leading to frequent and frightening “false alarms.”
- A middle-aged man who had a severe attack of vertigo appraised even mild feelings of imbalance as “I’m having another attack of vertigo – I’m in danger.” He made strong efforts to keep his head very still, closely self-monitored for signs of imbalance, and refused to travel far from home in case he had another attack.
Fears can be sweeping or quite specific, from animals, heights, and flying to being exposed to blood, injections, and injuries. Performance anxiety is a very real threat — facing audiences can feel just as terrifying as facing a pride of lions on open grasslands. Fears are real and can affect daily life, sometimes with dire consequences, even if the source of them is exaggerated or imaginary. Interpreting them correctly is the right path toward getting better.
In posts 13-15, I discuss some effective treatments. Exposure therapies are effective for anxiety disorders of all kinds, but they’re most effective for phobias, panic disorders, and obsessive-compulsive disorder (OCD).
Phobias and Evolution

Baby feels physical surface covering the cliff, but still hesitates to crawl to its mother, Wikipedia
Evolutionary scholars note phobias emerge at the developmental age when they become adaptive (or learned) — possibly regulated by hormones and level of stress experienced. Mumbai Zoologist Jalan wrote “Is There An Evolutionary Advantage To Phobias?,” ScienceABC, everyone is born with the two innate fears of falling and loud sounds. The rest is learned. Our parents, siblings, friends, TV, or social media teach us early to be scared of things to keep us safe.
In a famous 1960’s experiment by Cornell University psychologists Eleanor Gibson and Richard Walk, babies were hesitant to cross a visual cliff — a flat surface with the appearance of a drop part-way across — even when urged by their mothers. The babies discerned the drop and hesitated or moved to the shallow side to cross. The experiment showed healthy crawling babies can perceive depth. However, results didn’t indicate avoiding cliffs and fear of heights is innate.
As we get older, experience shapes our fears. A caregiver with an extreme fear of dogs passed it to a child who then grew up afraid of the friendliest, tail-wagging dog approaching him in the park. No longer afraid, he still avoids dogs.
Worse is an early violent experience. The good news is the more we experience something, the less likely we will remain scared of it, like watching a movie that keeps you up at night over and over again. Our parasailer above said, “I had never parasailed; he had been many times.”
It’s individual. Still a teenager, my husband joined the paratroopers for the wrong reasons (jilted by a girlfriend). The more he jumped out of planes, the more time he had to think about how crazy it was—and his fear kicked in. Not exactly a phobia, but close.
Phobias are Innate and Adaptive
Most common phobias are related to our forebears’ greatest threats
Image: Facebook
- Arachnophobia (fear of spiders) caused cave dwellers to stay clear of poisonous eight-legged creatures.
- Fear of heights (acrophobia) kept people from falling off cliffs — for a lifetime.
- Crawling infants show innate fears of falling and loud noises.
- Toddlers exploring become afraid of animals, monsters, and mom being out of sight (fear of strangers) — yet fears go away as the baby grows up and can start fending for itself.
An older woman terrified of cats her whole life couldn’t recall the source of her fear — nonetheless, the fear was potent and visceral.
Not until later in life does someone develop fears like agoraphobia (fear of outside world) — a phobia rarely seen in children but carrying a strong genetic factor.

The following chart compares fear and phobia:
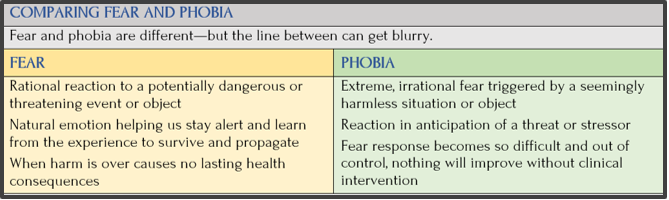
Source: Science ABC
Malfunction, Adaptation, or Genes?
There are many theories about the evolutionary role of primal phobia, states Mahak Jalan. Scientists believe they’re “a malfunction of our normal threat detection mechanism.” Most (but not all) phobias can be traced to a danger existing hundreds of thousands of years ago, says Jalen. In this view, phobias are malfunctions in some people, who develop an extremely strong reaction — like an allergy.
Another theory suggests phobias are adaptations of our stress response, rather than malfunctions. No matter how small, any phobia is a threat to us — be it snakes, spiders, heights, or even social embarrassment. A phobia still prevents us from getting too close to a poisonous snake or helps us avoid an uncomfortable situation. Jalen suggests a Darwinian natural-selection-of-the-fittest survivors who favored phobias because they kept them safe.
Studies suggest a genetic susceptibility to phobia, and many do develop the same phobia as their parents or siblings — due to common experience and environment. But we can still develop phobias they don’t have. Gradually the brain recognizes threats that become phobias — an explanation for why people may be phobic about spiders but not guns. These phobias did not develop in a single lifetime unless there was an earlier trauma.
Fear Extinction
There’s a process called fear extinction, defined in the scientific literature as a decline in fear responses due to multiple “non-reinforced” exposures. In his blog post, “Inside Fear and its Disorders,” Penn Medicine News, writer Steve Graff cites the following:
“Extinction is not forgetting a memory; it’s actually forming a new memory,” It’s learning a new safe association between the context or whatever cues were initially associated with danger. During extinction, you have a second form of learning happening that is competing with the original fear memory.” —David Connor, postdoctoral researcher, Department of Neuroscience, University of Pennsylvania
Steve Graff provides this example: Someone who’s been in an accident driving through an intersection fears getting hit going through the same intersection later. It requires driving through that intersection many times before the fear can be archived as a distant memory. Two nuances that help understand how this works in real life:
- Context matters. Extinction is strongest in the setting where it was learned and may not automatically transfer everywhere. A person may feel calmer in a therapist’s office but still reactive in a different environment.
- Original fear can return. Under stress, fatigue, or new circumstances, the old fear pathway can re-emerge (sometimes called renewal or reinstatement). This doesn’t mean extinction failed — it means safety learning needs reinforcement.
In conditions involving heightened threat sensitivity — such as anxiety disorders, trauma-related conditions, and at times bipolar disorder during periods of high stress — fear extinction can be harder to achieve or sustain. They find it difficult to extinguish fear because it has become generalized — lifted out of its context. Or the fear is a misplaced attribution, meaning a mistake in assuming the cause, preventing the brain’s record of the fear to be overwritten.
This isn’t about willpower, but about how reactive and adaptable underlying nervous systems are. At its core, fear extinction is a powerful protection mechanism: the brain’s ability to gradually recognize when fear is no longer required
Fear Extinction Deficits: A Study of nicotine addiction

Image: The Atlantic,Toshiro Shimada / Getty
Connor studies fear extinction and nicotine to find better ways to treat fear disorders. He says, “A lot of the circuits and brain regions that are involved with addiction are also highly associated with fear and anxiety-related behaviors. People with anxiety have higher rates of addiction because drugs, such as nicotine and alcohol, are perceived to provide short-term relief from their anxiety.”
But that may not be the case. In a study Connor co-authored in Neuropharmacology, nicotine may actually be making it worse. They studied the role nicotine plays during fear extinction.
- Mice were given two, mild shock stimuli in a cage and returned repeatedly to the same cage, minus the stimulus, to measure their fear extinction.
- Each time they were less scared, measured by how long they “froze” once back in the cage.
- Mice given nicotine took longer for freezing levels to decrease — they stayed scared longer.
“This suggests that nicotine can actually cause deficits in some forms of learning,” Connor said. “In this case, it’s in fear extinction learning.”
The researchers also found nicotine increased neural activity in the brain’s hippocampus and amygdala. Further, when the hippocampus, which signals the amygdala, was infused with nicotine, mice showed deficits in fear extinction. This suggests a hippocampal link between nicotine and extinction deficits — a potential target to alter fear extinction signaling in the future.
Phobia Prevalence
Phobias are the most widespread of all mental disorders, with 10%-30% of the population reporting a fear severe enough to disturb some functioning. About 19 million Americans have one or more phobias, ranging from mild to severe. Other data show phobias:

Image: VectorStock
- Afflict women more often and more intensely than men
- Co-occurs with chronic anxiety and depression
- Can trigger a fight-or-flight response (FFR)
Diversity of phobias, among participants in a study:
- 21% of women and 11% of men met criteria for any single phobia
- 5.4% of women and 1.5% of men reported multiple phobias
- 17.4% of women and 8.5% of men had situational phobias (lightning, enclosed spaces, darkness, flying, heights)
- 12% of women and 3% of men had animal phobias (spiders and snakes)
- No gender difference was observed in mutilation phobias (dentists, injections, injuries)
- Inanimate object phobias were more common in older individuals
- Fear of flying increased and fear of injections decreased in women, but not in men
Coming Up Next

In Post 10: Specific Phobia and Agoraphobia, I discuss specific phobias, social phobias, and agoraphobia.