On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
13. Why Anxiety Goes Undiagnosed — and Untreated

Photo: From Isabell Tenorio, “15 Self-Soothing Techniques To Manage Your Anxiety & Stress,” Your Tango
Getting a clear diagnosis for anxiety isn’t as straightforward as it seems. We know something feels off, but may not recognize it as anxiety. We’re not sleeping, or we brush it off as “just a tension headache.” Our thoughts take a negative turn and cycle repeatedly. Our body feels keyed up, suddenly overwhelmed — we just feel stuck.
And yet we persist in minimizing our anxiety, believing we’re overreacting. It’s just stress—a bad week, too much coffee, a work deadline. We push through it or explain it away. Sometimes years pass without realizing we shouldn’t be feeling this way. It’s not simply the human condition. We should and can feel better.
From DSM-5 to an Accurate Diagnosis
When we do decide to seek help, it’s not always clear how to proceed. Maybe we don’t want to go down the path of doctors and therapists. Maybe we don’t trust that something so internal can be diagnosed at all — after all, isn’t the world filled with stress, loss, and uncertainty? Who are we to expect relief?
The path to an accurate diagnosis can be slow, uneven, and at times confusing. Part of that has to do with how mental health is defined and classified. Clinicians rely on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition — mostly called DSM-5 — to guide diagnosis. It lays out criteria for different conditions, helping professionals distinguish between related disorders and determine when a pattern of symptoms crosses from a normal response into something more persistent or impairing.
But DSM is less a diagnostic test than an evolving framework. New editions appear every decade or so, and with each revision, categories can be folded together or separated out. What counts as a disorder is clarified, sometimes debated, and sometimes reconsidered.
So while DSM offers structure, diagnosis itself remains part art, part science — but mostly shaped by clinical judgment. There are several reasons why it can take a long time for anxiety to come into focus:
- No two people describe anxiety exactly the same. Clinicians rely heavily on self-report, which can be incomplete, imprecise, or defined by memory. A simple question — “When did this start?” — can be difficult to answer if the experience is rooted in childhood.
- Symptoms overlap across conditions. Anxiety can be part of mood disorders, dissociative or trauma-related experiences, personality patterns — or physical illness. What looks like one thing at first may, over time, reveal itself to be something else, or several things interacting.
- There are no definitive lab tests. Brain imaging can sometimes show patterns associated with mental illness, but it’s not yet used to diagnose anxiety. As these technologies continue to evolve, that may change. For now, the picture has to be built from experience, self-observation, and clinical judgment.
In sum
In practice, diagnosis emerges from professional expertise, DSM criteria, and, often, a period of careful observation and adjustment.
Many of us aren’t fully attuned to the discipline of self-reporting. We may not recognize what’s significant. We may second-guess ourselves, or feel embarrassed or ashamed. That’s one reason to write things down — even briefly: what we’re feeling, when it happens, what seems to make it better or worse. Especially when patterns repeat. These details, imperfect as they may seem, give clinicians a stronger basis to assess and treat what’s affecting us.
Getting the diagnosis right is a meaningful step so treatment can be more focused, individualized, and effective over time. But when a diagnosis is missed, the result is often prolonged symptoms — and unnecessary suffering.
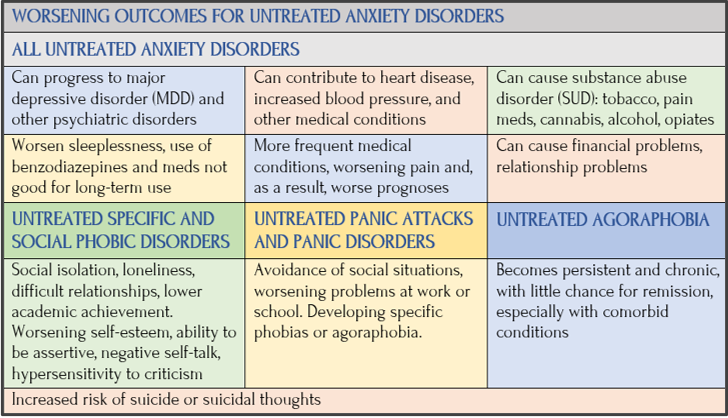
Untreated Anxiety Disorders
What happens when anxiety goes untreated is not abstract. It’s what follows from everything we’ve just seen—missed diagnoses, delayed care, systems that are hard to enter and harder to navigate. In post 2, I provided some statistics having to do with treatment outcomes. Three main points worth repeating:
- No matter how severe, all anxiety disorders can be treated, generally with short-term, effective, and cost-effective methods.
- Despite this, anxiety disorders are substantially under-recognized and undertreated.
- Approximately 1 in 4 people in need (27.6%) receive treatment.
This just cries out for a broad solution. So much suffering. So little relief. So many people don’t think therapy is for them, they don’t know where to go or who to turn to, they don’t realize they can be helped, and they may not even know they have an anxiety disorder to begin with. There’re certainly enough problems to go around. If you’re working overtime, money is tight, you feel stressed, and the stress is chronic, you may not believe there’s a way to feel better.
According to the World Health Organization (WHO), barriers to treatment include lack of awareness that anxiety is a treatable condition, lack of investment in mental health services, lack of trained healthcare providers, and social stigma.
Confronting the Source of Fear in Treatment
Chronic anxiety spikes when facing change, stress, or demands. Avoiding anxiety-producing situations may provide immediate relief, but without treatment this isn’t true over time. Yet, treatment is tough on anyone who must confront fears to get past them. With trust, guidance, and medication, the journey to health can feel less raw and more hopeful.

But DSM is less a diagnostic test than an evolving framework. New editions appear every decade or so, and with each revision, categories can be folded together or separated out. What counts as a disorder is clarified, sometimes debated, and sometimes reconsidered.
So while DSM offers structure, diagnosis itself remains part art, part science — but mostly shaped by clinical judgment. There are several reasons why it can take a long time for anxiety to come into focus:
- No two people describe anxiety exactly the same. Clinicians rely heavily on self-report, which can be incomplete, imprecise, or defined by memory. A simple question — “When did this start?” — can be difficult to answer if the experience is rooted in childhood.
Anxiety disorders are associated with a considerable degree of impairment, high health-care utilization, and an enormous economic burden for society. Although effective psychological and pharmacological treatments exist, many affected individuals do not contact health services for treatment, and of those who utilize these services, a high percentage is not diagnosed correctly nor offered state-of-the-art treatment. —WHO
Anxiety is a part of everyday life. Anxiety disorders are not. If not treated, anxiety disorders can become more intense (there’s evidence they improve with aging). Anxiety disorders are also highly comorbid — with other psychiatric disorders and substance use disorders (SUD) — and prognosis for achieving healthy outcomes worsens.
And because anxiety so often hides in plain sight—or is misread, minimized, or mistaken for something else—many people never reach the point where help becomes possible.
Diagnosing Generalized Anxiety Disorder (GAD)
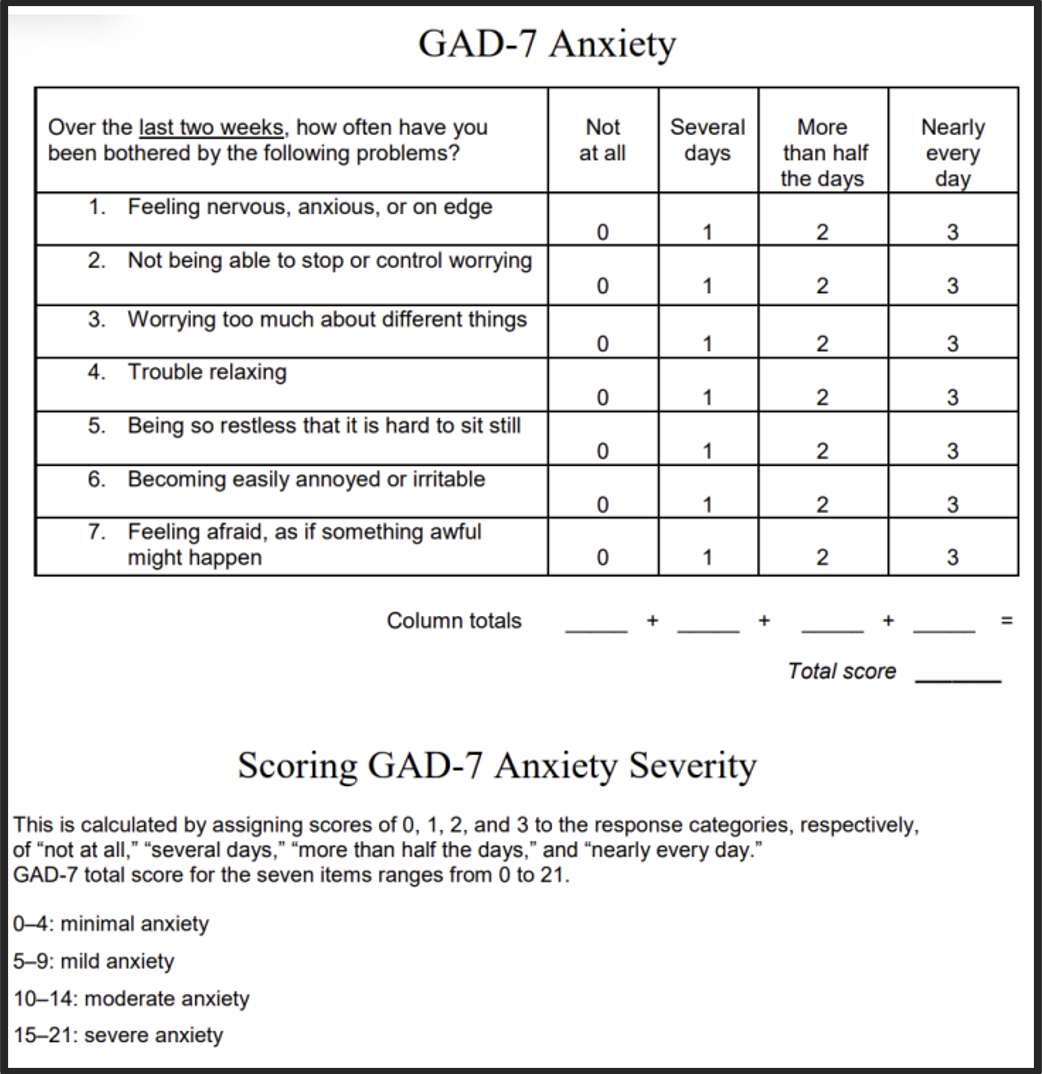
Primary Care Evaluation of Mental Disorders Patient Health Questionnaire (PRIME-MD-PHQ). Developed by Robert Spitzer, et al.
Generalized anxiety disorder (GAD) is both common and serious — and not easy to recognize for what it is.
DSM-5 offers structured ways to assess it. Primary care clinicians can administer brief screening tools like GAD-2 and GAD-7 — two- and seven-item questionnaires — to help gauge the level of anxiety. These paper-and-pencil tests can also help determine whether a referral for a more formal evaluation is needed. They’re also available for self-assessment, which can be a useful starting point.
For older adults, several additional self-administered assessments are available, including the abbreviated Penn State Worry Questionnaire, the Geriatric Anxiety Inventory, and the Adult Manifest Anxiety Scale. As noted by Sandra Swantek, MD, in an American Medical Association podcast [see post 9]: these tools can help capture how anxiety presents across different stages of life.
One point of confusion is language: clinicians don’t diagnose “anxiety attacks” as a formal condition. They diagnose anxiety disorders, specific symptoms, and panic attacks — terms that carry more precise clinical meaning.
Diagnosing Specific Phobia
Definitions of phobia have evolved over time. In DSM-6 (, 1994–2012), for example, phobic fear was described as excessive or unreasonable — triggered by encountering or anticipating a specific object or situation, and either avoided or endured with intense distress. Five subtypes were identified:
- Animal
- Natural environment
- Situational
- Blood-injection-injury
- Other
DSM-5 (2013-present) retains these categories but shifts the emphasis. Rather than requiring a fear to be labeled “excessive or unreasonable,” it’s now understood as out of proportion to the actual danger posed by the situation or its context.
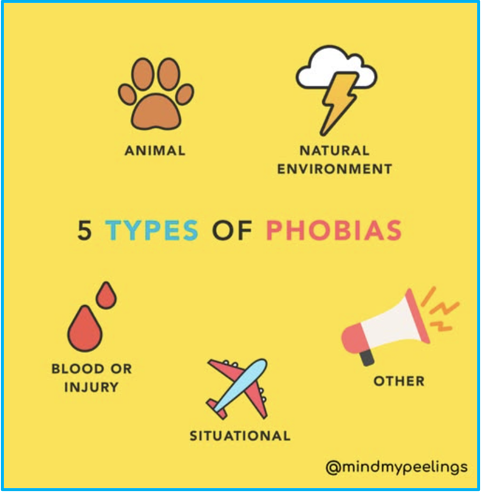
Graphic: Mind My Peelings, Facebook
That distinction matters. A fear of loud noises, for example, would be understandable in a war zone — but in everyday circumstances, the same response may signal a phobic pattern.
In practice, diagnosis depends on how narrowly or broadly fear presents:
- Specific phobia is diagnosed when fear is limited to a particular type or situation.
- Agoraphobia involves fear, avoidance, or behavioral change across multiple settings — typically at least two categories (such as open spaces, crowds, or public transportation).
- Social anxiety disorder (SAD) center more on anticipation and fear of negative evaluation than on the situations themselves.
- Panic disorder is diagnosed when panic symptoms occur outside of specific situational triggers or across a range of contexts.
Because symptoms can overlap, clinicians also consider related conditions such as separation anxiety, acute stress disorder (ASD), and post-traumatic stress disorder (PTSD). What appears to be a simple fear may, over time, reveal a more complex pattern.
Diagnosing Agoraphobia
Many symptoms of agoraphobia can mimic physical conditions — heart disease, gastrointestinal issues, or breathing problems — which can complicate diagnosis and delay treatment. Medical tests are often used first to rule out these possibilities.
The most effective way to a correct diagnosis is responding to a mental health specialist’s questions about your experience:
- Do you find it frightening or stressful to leave your house?
- Do you avoid certain places or situations?
- What happens if you find yourself in one of them?
As noted earlier, DSM-5 considers agoraphobia an independent diagnosis, separate from specific phobias or panic disorder. To meet criteria, a person must experience intense fear or anxiety — disproportionate to the actual threat — related to real or anticipated exposure to public or difficult-to-escape environments, such as:
Philip McKay “Agoraphobia,” digital art Artlimited, UK
- Being outside the home alone
- Open spaces (marketplaces, parking lots, large fields)
- Enclosed spaces (theaters, small offices, malls, elevators)
- Standing in lines or being in crowds
- Public transportation (cars, buses, trains, planes)
Diagnosis also requires these fears lead to meaningful changes in daily life — often through active avoidance. Symptoms must persist for at least six months and cause significant distress or impairment.
Importantly, agoraphobia is not diagnosed if the behavior is better explained by another condition — for example, avoiding public spaces due to a medical risk such as loss of consciousness related to cardiovascular disease.
Brain-Imaging Scans or Neuroimaging
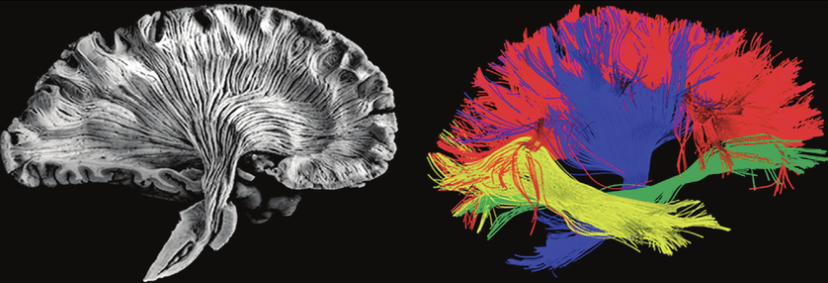
Dissection of human brain (Virtual Hospital) showing white-matter connectivity made up of axonal fibers. Artist rendering of bundle of fibers and water molecule trajectories moving along/across the bundle. Source: ResearchGate
Scientists are using brain-imaging technologies to get closer to brain activity and structure — and how that relates to mental health.
Newer forms of neuroimaging [see Glossary for MRIs, PET scans, and SPECT scans] are beginning to shape research in meaningful ways — and, at the edges, inform clinical thinking as well.
For example:
- Researchers have observed changes in brain activity in people with depression, panic disorder, and PTSD following psychotherapy — changes that, in some studies, resemble those seen with medication [American Psychiatric Association].
- Neuroimaging can also detect structural abnormalities — helping to distinguish psychiatric conditions from neurological disorders or brain tumors [NCBI/PubMed Central].
As these technologies evolve, they may begin to offer more objective support — patterns that can be measured, tracked, compared. If that happens, diagnosis may become more consistent, perhaps even more precise. But for now, it remains, in part, a human judgment.
Prevention of Anxiety Disorders

Graphic: The Plum Tree
I haven’t devoted much time to prevention because fear and anxiety are part of being human and not problems to eliminate. They help us navigate a complicated world. But when anxiety blossoms into something more consuming — phobia, panic, or persistent distress — it doesn’t always announce itself in ways we can easily recognize or interrupt.
In theory, prevention means paying attention to risk factors and early signs. As with any illness, earlier detection can lead to better outcomes. But in practice, this is harder than it sounds — especially when it comes to our own mental health.
In post 4, I shared Lena’s experience with panic disorder. There were hints — she was a worrier — but nothing that clearly signaled what was coming. Then came the incident: swept into the ocean, struggling to find her way back to shore, with no help in sight.
In retrospect, earlier attention to anxiety might have changed the course. But at the time, without a clear understanding of what she was experiencing — and with her concerns dismissed — she would have had to see what wasn’t yet visible.
That doesn’t mean we ignore the early signals. If we notice patterns — heightened stress, emotional reactivity, irritability, or withdrawal — it’s worth paying attention. Not as diagnosis, but as signals.
Healthy Living
I’ll return to healthy living — nutrition, exercise, sleep, and substance use — in later posts. For now, it’s enough to say that our daily habits can either steady us or mask symptoms or make them worse.
These habits don’t prevent anxiety in any absolute sense. But they can function as a kind of early barometer — showing us when something is changing, and perhaps prompting us to seek support sooner, while things are still more manageable.
Deterrence and Patient Education
We need to improve how we manage emotions that overwhelm us — to notice when we’re denying or suppressing what’s happening, or when our thoughts slip into repetitive, exhausting loops.
We will have better prognoses if we can do this. If we can identify our symptoms early, intervene promptly, access resources and mental health professionals, and be open and committed to our treatment plans. Yet, even with all of this, anxiety is not easy to prevent. We just have to keep trying. Once we begin to see the pattern — maybe not at first — it becomes something we can work with.

A U.S. Task Force on Preventing Anxiety
Photo: Vecteezy
The U.S. Preventive Services Task Force (USPSTF) — a panel of volunteer experts in prevention and evidence-based medicine — aims to improve health nationwide by making recommendations about screening and early intervention. In 2023, the task force recommended screening adults ages 19-65 for anxiety disorders, suggesting use of tools (like GAD-7) as part of routine care.
It’s a meaningful step. For a long time, anxiety has been minimized — treated as a personality trait or a private burden rather than a condition worthy of attention. Bringing it into regular, annual medical check-ups can change that.
It’s not yet clear how widely these recommendations are being implemented. I recently had my annual physical, and no such screening was offered. In practice, it often still falls on the patient to raise the issue — to say, something isn’t right — which isn’t always easy to do. That’s because, sometimes we don’t:
- See our symptoms clearly.
- Expect much from a medical visit that’s often quite brief.
- Raise psychological concerns due to embarrassment or shame.
- Realize talking to nurse practitioners is a good place to begin.
- Realize there are effective treatments
Take your pick — it could be any number of these issues. For this reason, advocacy matters — both within the medical system and in our own lives. We need to pay attention and speak up when we can. And when we can’t, we should ask someone we trust to help us do that.
For me, it was a psychotherapist. In the middle of a session, she stood up, walked to her desk, wrote a name and phone number on a piece of paper, pressed it into my hand, and said, “It’s time. You need antidepressants.” I was taken aback. It wasn’t expected, and I thought she might be overreacting. But she wasn’t. Once the medication began to take effect, I felt better and more able to take next steps in managing my anxiety.
Coming Up Next