On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
11. Anxiety Attacks vs Panic Attacks vs Panic Disorder

Before writing on anxiety disorders and phobias, I planned to focus on anxiety and panic attacks. Largely because these terms are frequently Googled — so people are seeking information — and because such extreme and temporary takeovers of our bodies warrant a closer look at why this happens. Especially because there seems to be a cognitive and emotional separation. I understand what I’m going through isn’t rational, but I can’t control it anyway.
I also have first-hand experience in anxiety, anxiety attacks, insomnia, the physical sensation of dread, and a feeling of losing control. But I don’t get panic attacks.
This tell me there’s a difference between anxiety and panic attacks, despite web sources conflating the two conditions. In this post, I’ll try to understand their distinctive features, along with the underlying anxiety that makes them possible. Here’s my story:
My Anxiety Attacks
My anxiety attacks start with my gut filling up with a substance, like curdled milk with dollops of cleaning fluid (undoubtedly cortisol [post 5]). This uncomfortable feeling is with me for a while before a sense of dread starts spreading like tingling lava through my head, down my neck, and into my chest — a feeling akin to being caught stealing my son’s college fund while the FBI close in and take me away under the careful watch of my coworkers and neighbors.
Physical feelings are unsettling. Psychological ones, humiliating. It takes place in slow motion, while I remain in full possession of my thoughts about what’s happening. I don’t think I’m having a heart attack nor I’m about to die. The anxiety attack seems to last forever, even if only 30 minutes have passed. Unlike a panic attack that ascends and descends the high-anxiety bell curve in under an hour, the anxiety attack doesn’t necessarily diminish over time.
In fact, the only way it ends for me is when I take active, cognitive, and physiological control. I exert cognitive effort and will to change its course, because my natural inclination is to start chugging wine. The first step is stock-taking of what’s happening (not as obvious as it sounds). I stop what I’m doing, consider what triggered me, think on it, narrow it down, and then figure out counter measures to calm my body down. If efforts fail or I’m too far gone, I might take half a Xanax — which I try not to do (fear of dependency).
A word on Xanax. I always keep a prescription — but can go long periods without taking any. Just knowing it’s there is sometimes enough.
Overall, I’m fairly successful at attacking the attack. Once or twice I’ve been lucky enough to have an anxiety attack while with my therapist, who I can then observe observing me. I pay close attention to what he tells me to do in the moment. He has said many times, if I breathe deeply, in and out, engaging my diaphragm, it becomes physically impossible for my anxiety symptoms to sustain. It’s one or the other. Anxiety and shallow, sped-up breathing OR deep breathing and lessening anxiety.
This removes fear from my anxiety attacks. Fear is a purely physical reaction to a stressor. But once I recognize the pattern, I also know I’ll be okay. It’s an awful feeling, for sure, but I can recognize my agency in reversing course. Reversing anxiety attacks takes practice (awareness, radical acceptance, breathing, healthy distractions), excellent therapy, antidepressants, and an emergency half Xanax. And maturity.

Photo: Stockcake
My phobia is claustrophobia that builds over time. Especially in crowded elevators after the third person has stuck their arm through the closing doors causing the doors to bounce open yet again. Squeezing in and pushing us back. Once I exclaimed rather loudly, “Can you please let the doors close!” It was surprising, especially that it came from me. This is not a phobic reaction to elevators or heights — neither affects me. But not being able to move or escape is my version of torment.
Yet even this isn’t always the case. When commuting to work, I often rode packed subway cars. I didn’t care for it (who would?), but the tension only rose when the doors couldn’t close because people were squeezing themselves in. The train had to be moving for me to be okay.
Once I was trapped and unable to move on a crowded street during some event. That might have turned into a panic attack if I hadn’t aggressively pushed my way through unyielding seas of people. As soon as I was free of them and could move, I was fine. I’m now more careful to anticipate this, and it hasn’t reoccurred. Again, when younger, I went to a fair share of rock concerts teeming with people. Only if they surged did my claustrophobia rear up.
Everyone Else’s Anxiety Attacks, Panic Attacks, and Panic Disorder
Anxiety attacks stem from anxiety, with symptoms of worry, distress, fear at different levels of intensity and augmented by any number of other, common psychiatric disorders. Incidents of anxiety attacks and claustrophobia are clearly related symptoms of generalized anxiety disorder (GAD).
For others with a specific phobia, they may indeed be triggered into experiencing an anxiety or panic attack when encountering or fearing an encounter with the source of their phobic fear. The cliché about fainting at the sight of blood is actually a real thing for a lot of people. Some find themselves in a condition of high anxiety going to the dentist and need to be sedated to have their teeth cleaned. Others, even those who aren’t superstitious, may cringe at a black cat crossing their path, without prior awareness they harbored such a fear.
In addition to GAD and specific phobias, comorbid psychiatric conditions add to the likelihood of anxiety attacks occurring: panic disorder, separation anxiety disorder, social anxiety disorder (SAD), agoraphobia without history of panic disorder, post-traumatic stress disorder (PTSD), and obsessive-compulsive disorder (OCD).
Panic Attacks and Panic Disorder
I wrote about two people experiencing panic attacks [post 4], whose sudden bursts of terror, in the absence of current danger, was an uncomfortable experience for them. Their symptoms were mostly physical, ranging from “I need to get home now” to heart-attack level terror minus the heart attack. It’s sudden, scary, with hyperventilating and a fast pulse — a panic attack can peak in minutes and take 10-60 minutes to subside. The result is a helpless feeling of being out of control and feeling extreme, enervating fatigue.
Panic attacks can come up without warning and at any time — when driving a car, shopping, sleeping, or working. If they occur frequently, a person may’ve developed a panic disorder. The person pretty much never wants to have this experience again. Avoidance brings on a host of other problems — disrupting routines and affecting relationships, school, or work performance
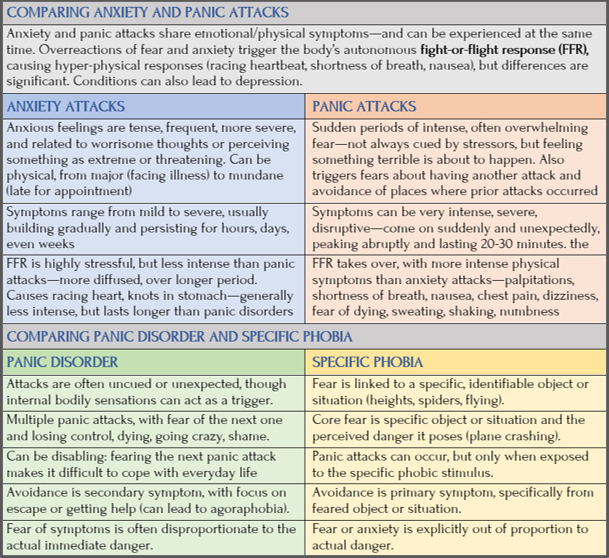
According to Johns Hopkins Medicine, panic disorder is characterized by surprise panic attacks that recur frequently and are “abrupt and intense surges of fear.” Repeated and unexpected, panic disorder is accompanied by physical symptoms, like palpitations, shortness of breath, nausea, chest pain, dizziness, and fear of dying. Research suggests panic disorders involve the fight-or-flight response (FFR). Hopkins Medicine: “Yet the alarm system is set off at inappropriate times, without present danger and for no apparent reason. The resulting panic attack is the sped up heart or rapid breathing of the alarm system.”
There may’ve been past situations triggering a panic attack, but mostly there’s no knowable cause for the fear. Because panic disorder is diagnosed when panic attacks are frequent, the person has a high degree of worry about when and where the next one may happen. If severe enough, it can develop into a phobia keeping the individual at home (agoraphobia), though that’s somewhat rare.
People with panic disorder have a stressful existence, fearing they won’t be able to find help or will be forced into a situation that will trigger the next attack. It’s common for people in this situation to relieve stress with alcohol/drugs.
Causes of Panic Disorders, Phobias, and Agoraphobia
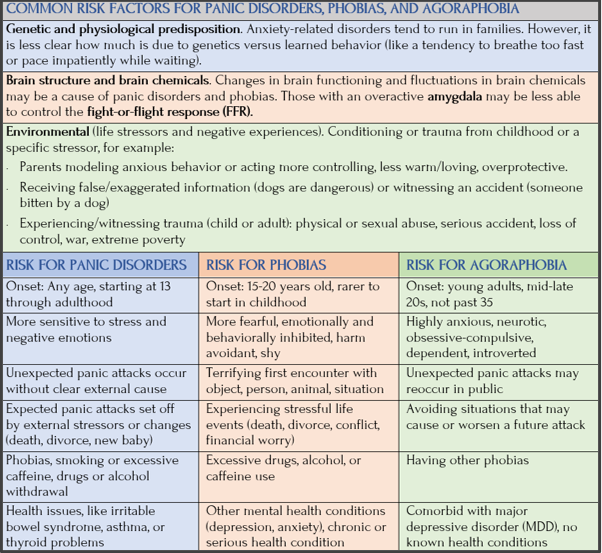
Although causes are unclear and in dispute, anxiety-related disorders like panic disorder, phobias and agoraphobia arise from a complex interaction of biological and environmental factors, worsening of lifelong behaviors, and personality factors, as I show in this chart:
Prevalence of Panic Disorders
Panic attacks are common and can happen to anyone. From a national statistical survey estimate of U.S. adults ages 18 or older:
- 4.7% experience panic disorder at some time in their lives, with 2.7% in the past year
- Prevalence was higher for females (3.8%) than for males (1.6%)
- Degree of impairment ranged from mild to serious (44.8% serious, 29.5% moderate, 25.7% mild), with no differences based on age or gender distribution
Estimate of U.S. adolescents ages 13-18:
- 2.3% experienced panic disorder in the past year, with 2.3% having severe impairment
- Prevalence was higher for females (2.6%) than for males (2%)
Photos: Your Tango, fizkes / Getty Images; “How to help someone having a panic attack: first, stay calm,” Happiness.com


Genetic Vulnerability to Panic Disorder
As with most mental health conditions, there is no simple genetic trail. It’s mostly about genetic vulnerability and how that mixes with stressors and dispositions to be realized into a disorder. Having said that, researchers have found strong causative links, according to Wikipedia: “Neurochemical dysfunction plays the most prominent role in genetic cause for panic disorder.”
Genes contribute significantly to panic disorder, but so too do neural networks. Here’s what they know (from NIH):
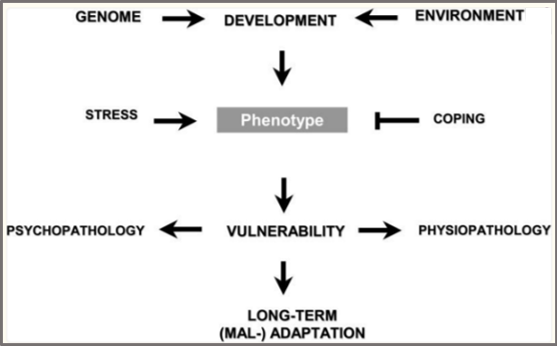
Diagram of genetic factors interacting with developmental stress to impact vulnerability to develop anxiety and other psychopathology.” From Seth Norrholm and Kerry Ressler, “Genetics of Anxiety and Trauma-Related Disorders,” PubMed Central/NIH
- Heritability: Risk estimates are 30%-40% from genes.
- First-degree relatives (parents, siblings) have a substantially higher risk (3x-17x) of developing the disorder.
- Complex inheritance: It doesn’t follow simple genetic patterns, suggesting many genes with small effects interact.
- Neurotransmitter systems: Implicated genes often affect serotonin, dopamine, and GABA systems, plus other biological pathways, pointing to predispositions interacting with environmental stressors.
Even when I work hard at reading the science, the science hovers above. So I read it as poetry to gain a sense of meaning if not actual, conceptual understanding.
Here’s what I mean by poetry:
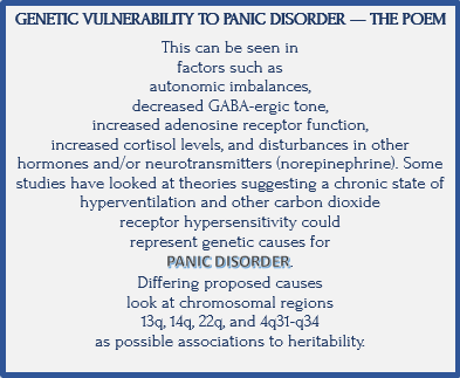
Text selected from Wikipedia and formatted into a poem by Jan Swan
Coming Up Next

In Post 12: Anxiety Disorder Risk Factors and Symptoms, I’ll discuss anxiety and panic attacks/disorder risk factors and symptoms.