On Anxiety and Panic Disorder
Show Table of Contents
INTRO
FEAR VS ANXIETY VS ANXIETY DISORDERS
- Emotional Health vs Mental Health
- Fear vs Anxiety
- Personal Journeys with Anxiety and Panic Disorder
- Fear, Anxiety, and Fight or Flight
- The Evolutionary Role of Anxiety
- When Anxiety Drifts to Disorder
- The Ancient Advantage and Current Anguish of SAD
PHOBIAS, ANXIETY / PANIC ATTACKS
- Phobias and the Rapid Onset of Fear
- Specific Phobia and Agoraphobia
- Anxiety Attacks vs Panic Attacks vs Panic Disorder
- Anxiety Disorder Risk Factors and Symptoms
- Why Anxiety Goes Undiagnosed — and Untreated
TREATING AND COPING WITH ANXIETY
17. Being Attuned to the Brain-Mind-Body Connection

Source: Andrés Gómez-Emilsson, “Visualizing Tactile Sensations,” Qualia Research Institute
We didn’t evolve to be calm. We evolved to survive. For hundreds of thousands of years, that meant living in harsh environments where danger was immediate and often fatal. Survival depended on sharpening our attention by fear. Anxiety kept us alert. The clan extended beyond immediate kin — for protection from other clans and, for continuity, to propagate the species.
As sure as we have five-fingered hands, thinking and feeling regions of the brain, and senses attuned to the environment, we have core emotions: fear and anxiety, anger and joy. Those emotions didn’t disappear when the threats changed. They remain an essential part of the human condition.
Now the dangers are different — no longer a predator at the clearing’s edge, but ongoing, often unresolvable pressures from work, uncertainty about our futures, disappointment, and loss. The body doesn’t distinguish cleanly between these ancient and modern worlds. We’re left to make sense of signals designed for another time.
This causes many of us to feel a loss of control. Rain dances don’t bring water to dry fields. Lucky shirts don’t cause our team to win. And yet we keep asking: do we control any of this — war, racism, the climate? Do we have control there?
Illusion of Control
As we moved from survival in the wild to life in organized societies, we developed rituals and practices that gave us a sense of influence over what lay ahead. We held onto a mistaken belief: that we could shape outcomes far more than we actually can.
The illusion of control, a term coined decades ago by Harvard psychologist Ellen Langer, describes this tendency to overestimate our influence over events that are, in reality, uncertain or governed by chance. At times, that belief can be useful. It can motivate effort, persistence, a willingness to try.

Dan Pilat and Sekoul Krastev, “Why do we think we have more control over the world than we do?” Decision Lab
But it can also misdirect us. We act on this illusion bias, deluding ourselves into believing we can control outcomes, timing, other people, while turning away from the more demanding work of changing how we respond. We expend energy anticipating or hoping for a different outcome, rather than engaging with what is actually unfolding. The pull is toward what feels easier or more certain, even when it leads nowhere productive.
At its worst, this illusion can make us passive — waiting for something good to happen, relying on chance, or choosing easy ways out rather than thinking through what might actually help. We tell ourselves things will fall into place on their own — that we’ll meet the right person by accident, that something unsustainable will somehow work this time, that change will come without requiring much from us.
But you don’t meet the person of your dreams by waiting for coincidence to deliver them. You don’t lose weight on an ice cream diet. And if you’re housebound, you don’t climb onto a rollercoaster and expect everything to feel different.
Left unchecked, this illusion can pull us toward decisions that feel reassuring but don’t hold up — keeping us invested in what isn’t working, as if wanting it badly enough might make it so. It might even put us at risk for making poor decisions, pinning our hopes on magical thinking, or — in the case of gamblers — keeping us at the card table well after we’ve already lost a fortune.
Letting go of that illusion shouldn’t mean resignation, but reorientation — toward what is actually within reach.
we need one another

Henri Matisse, The Dance I, 1909
If you have anxiety attacks like I do or, worse, panic attacks, if you’re climbing 25 flights of stairs to avoid the elevator, then try the many techniques designed across the centuries and decades by people searching for more wholeness in a fractured world. Keep up with new science on the brain-mind-body connection, so you don’t leave the body behind. Or the brain, for that matter. Aspire to take a single step each day to get a little bit better.
This post gives information about ways of getting in tune with what our bodies need to be healthy and what we need to find peace, to grow, to prosper as individuals, in our relationships, in our pursuits.
If we understand how our body and emotional/mental states are not just intertwined but fused, perhaps we’ll hone our instincts to care more about our bodies.
Newer therapies have less evidence behind them for predicting, preventing, and treating mental illness than cognitive behavior therapy (CBT) and other evidence-based therapies (EBTs). The newer approaches maybe can help someone who hasn’t been helped by traditional therapies. If we can stop believing it will all work out, there are ways to distance ourselves from long-term harmful behaviors. Not just substance abuse, but avoidance, distraction, or other distancing behaviors taking us away from ourselves — not toward or forward.
Brain-mind-body science resides firmly within 21st-century biomedical, psychological, and neurological research. This is important for our future cognitive, emotional, and physical health.
Interoceptive and Exteroception Stimulation Therapies
A body signal appears — and we decide what it means. A racing heart is danger, dizziness is something wrong, the chest tightening is a warning that something is about to happen. Sometimes we’re right, but often, not. We’re not reading the signal itself. We’re reacting to our interpretation of it. Add to that, deluded interpretation, and that’s where things begin to spiral.
In reading for this post, I encountered the concepts of interoception, exteroception, and related therapies. The concepts seem to offer insights into how our brain-mind-bodies function. They relate to our unconscious, automatic fight-or-flight response (FFR) [see post 5] in how our bodies sense and respond to sensations (internal/external) before conscious awareness kicks in. A third domain to interoception and exteroception is proprioception.
To define this, I found “Experiencing our body: The role of interoception,” by Emma Herms, a PhD student in psychological and brain sciences, Indiana University Bloomington, ScIU blog. Looking at a photo of a woman underwater, she explains the three domains [paraphrased]:
- Exteroception refers to the body’s response to the external environment, like auditory and visual information. This would be the hum of moving water that dampens other sounds.
- Proprioception refers to the body’s position and movements. This would be arms and legs moving while treading underwater.
- Interoception refers to the body’s internal state, like our heartbeat and digestive signals. This includes feeling a lack of air in the lungs.

Emma Herms, “Experiencing our body: The role of interoception,” Indiana University Bloomington, ScIU blog.
Avoidance and Safety Behavior in Response to Anxiety Disorders
By focusing our attention, most of us with anxiety could avoid external stressors, but it’s much harder to avoid our own bodily sensations — like a faster heart rate, dizziness, sweating, feeling hot or cold, or back or stomach pain. Misinterpreting the meaning of these body sensations can trigger emotional and physiological reactions of fear and anxiety. These feelings, in turn, motivate avoidance and safety behaviors — that is, ways to cope to reduce anxiety and fear when feeling threatened.
While useful in the short term, avoidance and safety behaviors may become harmful (maladaptive) over the long term by prolonging anxiety and fear of nonthreatening situations — a common problem in anxiety disorders. In the long-term, avoidance results in ineffective and harmful behavioral changes and blocks positive ones, like learning about the true nature of the threat and dealing with it more directly.
This is why I wanted to learn more about these bodily sensations. Avoiding what potent emotional cues are telling us puts us at risk for being out of touch with our bodies, from within and without ourselves. It means we might try the wrong solutions to improve our mental health, because we’re not attuned to what we actually need.
Imagine you become aware of your heart beating faster (interoception) and start to gather other contextual information. You smell fresh baked bread and hear the bustle of a busy restaurant (exteroception). You also notice your knees are bent sitting in a booth (proprioception). Maybe you are sitting across from a date (exteroception). With this context, you might interpret your increased heartrate as nervousness. In this example, I have described exteroception, proprioception, and interoception as conscious experiences, and sometimes they are. However, our brains are constantly tracking and integrating information from these three domains even when we are not consciously aware of it! —Emma Herms, Indiana University Bloomington, ScIU blog
Interoception
Interoception involves sensory perception from inside the body (changes in heartrate, respiration, temperature, tension, pain). These sensations tell us whether we’re hungry, thirsty, unwell, or sleepy. Interoception helps us recognize when we’re feeling emotions (positive or negative, mild or intense):
- Emotional valence is the value associated with emotions along a continuum from pleasant to unpleasant and from attractive to aversive.
- Emotional arousal is a continuum of the emotion’s intensity and strength from high to low.
For example:
- Happiness is characterized by pleasant valence and relatively high arousal.
- Sadness is characterized by unpleasant valence and relatively low arousal.
Valence–Arousal Model of Emotion: Emotions vary along two dimensions: valence (how pleasant or unpleasant an emotion feels) and arousal (how energized or activated it feels), helping explain why emotions with a similar tone can vary in intensity.
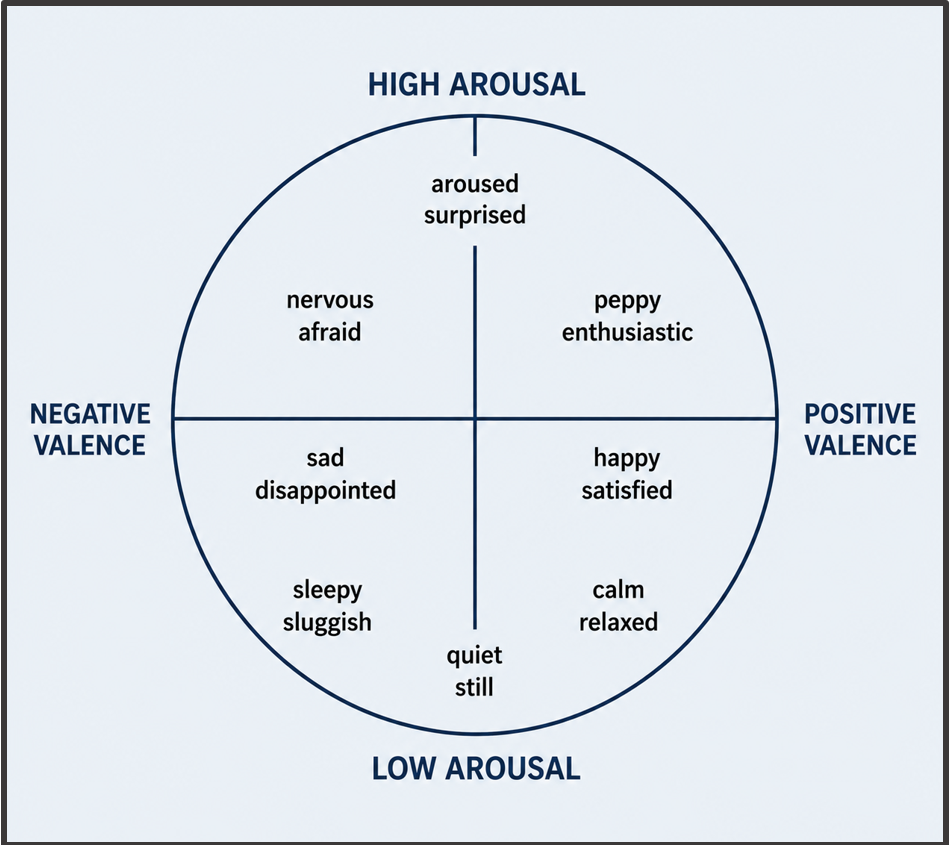
Adapted from Lisa Feldman Barrett, “Valence-Arousal Model and Its Application to Understanding Emotions.” Emotions in Everyday Life, 1993
Many consider interoception to be a “sixth” sense for understanding these internal sensations on a moment-to-moment basis. Here’s another way to look at emotional arousal:
- Good interoception means you feel hungry and get a snack. Or you feel a racing heart and breathe deeply.
- Low interoception means you go all day without eating. Or you have a surge of anxiety fearing you’re about to have a heart attack.
Evidence suggests high/low interoception in one domain doesn’t mean high/low interoception overall. You can have high interoception recognizing hunger, but low recognizing emotions.
Studies of interoception and mental health show being too aware of but misinterpreting internal body sensations can contribute to anxiety disorders. Other links are being researched between interoception and depression, obsessive-compulsive disorders (OCD), trauma disorders, substance use, and suicidality.
Interoceptive exposure exercises (IEE): Interoceptive exposure to feared stressors is one of the most effective psychological treatment for anxiety that stems from fear of internal body sensations. IEE brings about changes targeting various physiological and psychological symptoms — and threat appraisals. The exercises re-create in a safe space the body symptoms associated with the stressor and encourage the person to maintain contact with the stressor without avoidance or distraction. Here are select examples from Psychology Tools of IEE by body system, followed by the suggested exercise:
- Respiratory system (shortness of breath, throat tightening): “I can’t breathe,” or “I will pass out.” IEE: deliberate hyperventilation, such as breathing rapidly for one minute
- Cardiovascular/circulatory system (heart racing, sweating): “I’m having a heart attack.” IEE: intense physical exercise, such as running on the spot
- Muscle tone (muscle tension, tightness, shaking, imbalance): IEE: applied muscle tension
- Psychological system (feelings of unreality): “I’m going mad,” or “I’m losing my mind.” IEE: staring in a mirror for an extended period
EXTEROCEPTION
The opposite of interoception, exteroception is the body’s external perception, mediated through our five senses — sight, sound, touch, smell, and taste — plus temperature, pain, and physical symptoms like heart rate and respiration. Exteroception strongly affects our physical and psychological wellbeing. In fact, it’s important for any organism to be able to adapt and respond to their external environment. In exteroception, specialized sensory cells, called exteroceptors, respond to objects and occurrences in the environment. The brain’s hippocampus aids exteroception and encodes, stores, and retrieves long-term memory.
Exteroception Stimulation Therapy (EST)
Exteroceptive stimulation therapy refers to the external stimulation that affects the sense organs — eyes, ears, skin, nose, and tongue. The therapy uses multi-sensory stimulation methods to treat a number of anxiety disorders, including sensory processing disorders, anxiety, and trauma-related disorders.
Exposure to nature reduces stress and anxiety levels. Listening to calming music or engaging in relaxing activities may have a positive effect on mood and mental states. Other therapies that help exteroception include sensory integration therapy (SIT) and exposure therapy. In Psychology Lexicon, EST includes stimuli by sense:
- Visual: colors, shapes, movement
- Auditory: sounds, music, speech
- Tactile: temperature, pressure, texture
- Olfactory: scents and odors
- Gustatory: flavors and tastes
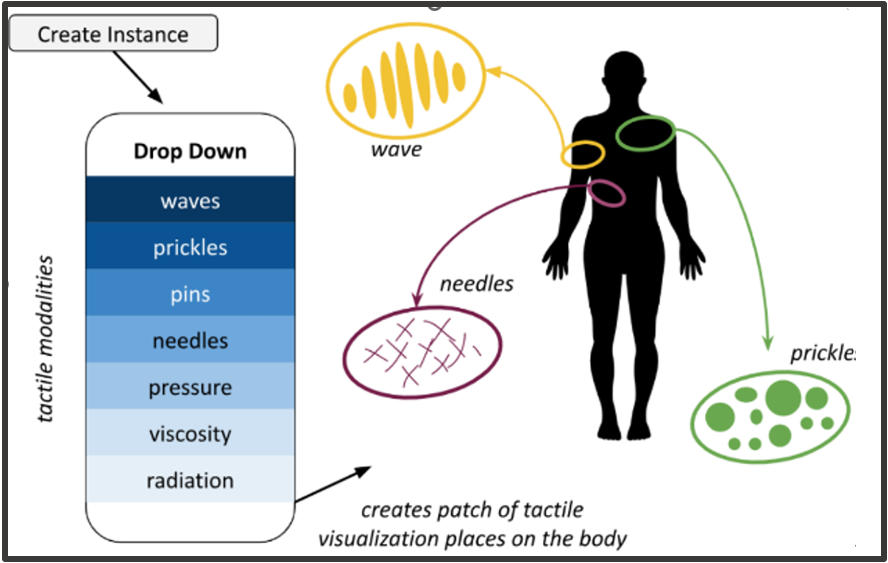
Riccardo Volpato, et al., “Visualizing Tactile Sensations,” Qualia Research , Psychology Lexicon
Both interoceptive exposure exercises (IEE) and exteroception stimulation therapy (EST) work for many anxiety conditions, including panic attacks and panic disorder, trauma, health anxiety (worry about a medical condition), chronic pain, chronic dizziness, and sensory processing disorders. IEE and EST are effective adjunct therapy with other forms of therapy. Recent data indicates that outcomes improve as these exercises are practiced more frequently, for longer, and with greater intensity, leading to greater reductions in anxiety.
Proprioception: Proprioception refers to the ability to sense your body in space as related to gravity. Proprioception relies on the vestibular system, which is housed in the inner ear and in the joints of your body.
Neuromodulation and Neurostimulation Therapies
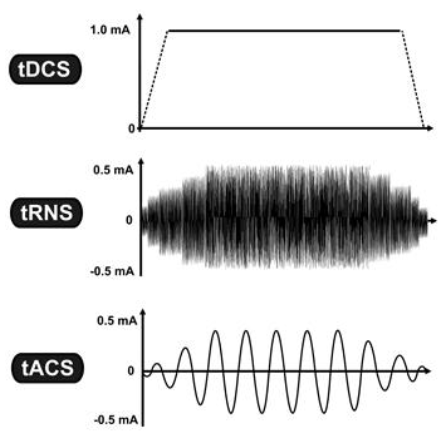
Three common forms of transcranial electrical stimulation: tDCS uses steady current, tRNS uses randomly fluctuating current, and tACS uses rhythmic alternating current. The vertical axis shows current strength (mA), and the horizontal axis shows time. Wikipedia
Early electrical stimulation experiments that started in the 1820s and have rapidly evolved over the past two decades into brain modulation research, applied to numerous physical and psychiatric disorders. Neuromodulation therapies alter the way nerves carry information to and from the brain by delivering electrical stimulation or chemical agents to specific neurological sites in the body. These therapies have been used for many wide and wonderful purposes, including preventing cluster headaches, reducing tremors, repairing spinal cord damage, decreasing pain, and increasing mobility. Also, they are being applied to psychiatric conditions for people who have treatment-resistant depression (TRD), anxiety disorders, anxiety attacks, PTSD, OCD, and panic disorder.
Neuromodulation is an umbrella term that emphasizes a broader, slower change in brain function in disease treatment.
Neurostimulation (brain stimulation) usually refers to the electromagnetic approaches to neuromodulation. This is an exciting area of further research and development. Here are some brief descriptions of neurostimulation therapies:
- Transcranial magnetic stimulation (TMS), a non-invasive procedure using magnetic fields to stimulate the brain’s nerve cells, is being studied for anxiety disorders and may reduce symptoms in some cases. It works by sending consistent magnetic waves to the brain’s prefrontal cortex. TMS sessions take 40 minutes, given daily over a period of 3-4 weeks.
- Repeated TMS (rTMS) sends intermittent magnetic pulses to target brain regions thought to be involved in anxiety disorders. rTMS is not an approved treatment for anxiety disorders, probably because of few conclusive research studies. There are, however, positive reports of rTMS improving symptoms in panic disorder — though not offered in clinical practice.
- Electroconvulsive Therapy (ECT) is a noninvasive therapy that stimulates the brain with electric current to relieve severe mood disorders — or when a rapid response is necessary for those at risk for suicide. ECT affects brain chemistry, which can quickly improve symptoms. Studies report improved depression symptoms in 70%-90% of individuals. Still, though safe and effective, it’s underused — possibly due to stigma and misinformation, lack of availability, or concerns over side effects. Data regarding ECT’s efficacy in anxiety disorders are limited — science hasn’t found the mechanism and focal targets for ECT to treat anxiety.
Ketamine Infusions for Anxiety
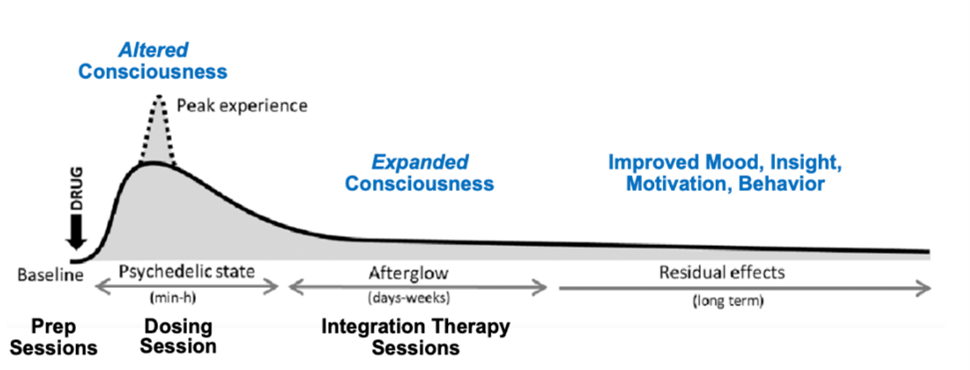
“Psychedelic-Assisted Therapy,” Art of Counseling
In ketamine-assisted psychotherapy (KAP), prescribed doses of the drug ketamine, along with psychotherapy, are increasingly being used to treat treatment-resistant depression (TRD) and anxiety. Even after a first ketamine infusion, there can be significant improvement in anxiety symptoms. It is also showing positive results for treating obsessive-compulsive disorders (OCD), post-traumatic stress disorders (PTSD), and physical pain.
While its primary use is as an anesthetic (for humans and animals), ketamine also has rapid analgesic and hallucinogenic effects, creating interest in its use as an antidepressant. Newer studies aim to harness its psychedelic effects to bring about altered states of consciousness that augment the benefits of psychotherapy in a short time — even within a few hours.
Researchers understand ketamine’s role in re-wiring the brain’s neural connections by enhancing neuroplasticity — regulating thought patterns and removing negative thoughts from the brain.
KAP is still controversial, but appears to have a high success rate. Studies suggest more than half of the people with mild to moderate symptoms achieve significant relief after a single infusion, and many more find relief after two or three intakes.
“Ketamine Assisted Psychotherapy,” Integration Therapy
While fast-acting, KAP may take time to fully relieve anxiety symptoms. Typically, the first phase is a series of six infusions over two-three weeks, followed by long-term maintenance that may include occasional booster infusions, as needed.
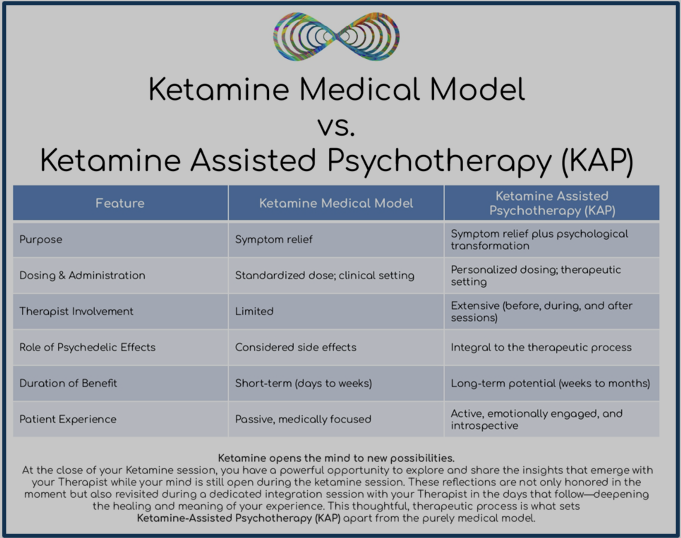
For the curious, here is a comparison of katamine’s medical and its psychotherapeutic use:
Brain-Mind-Body Interface Disorders

“Mind-body connection is built into brain, study suggests,” Newswise, Washington University. Graphic: Sara Moser
Increasingly, researchers and clinicians are paying closer attention to the brain–mind–body connection — recognizing that physiological and psychological processes are not separate tracks, but interacting systems (as in the fight-or-flight response to stress).
The following information is from Neuropsychiatry online:
Some have proposed a new way of thinking about this overlap: brain–mind–body interface disorders — conditions shaped by the continuous interplay between bodily processes, emotional states, and cognitive patterns.
In this view, treating physical symptoms in isolation might miss something, and better results may come from considering psychological processes —
where medical and mental health practitioners work together. And where processes like biased attention, fear avoidance, catastrophizing, dissociation, or alexithymia (emotional blindness) are understood as part of the condition itself, not secondary to it.
The authors describe a range of conditions that might fit within this framework — including chronic pain, brain–gut disorders, fibromyalgia, and persistent symptoms following brain injury — while noting that others, such as Alzheimer’s, Huntington’s disease, or epilepsy, don’t appear to benefit from this lens. Still others — including depression and severe panic with strong bodily symptoms — may be better understood through it.
The significant change with this approach is not just how things are classified, but individual experience. It may be the first time symptoms are recognized as real — not just physical or psychological, but both. Treatment, in turn, becomes more integrated: physiotherapy alongside psychotherapy. Sadly, the brain–mind–body approach lacks a clear medical home. Patients and clinicians can find themselves caught between categories — unsure where a problem belongs, or how it should be treated (or paid for, due to rigid insurance categories).
The idea itself is intuitive. But its implications are big, asking more of clinicians, systems of care, and patients and families. It seems that individuals and close family will increasingly need to take an active role in shaping how their condition is understood and treated.
Some of us may need to be the tails wagging the dog — pushing for care that reflects not only have we feel, but how our bodily systems actually work.
Think about something as ordinary as a stress headache. I have them. They hurt.
Coming Up Next
By remembering the clans of our forebears, we can remember we need each other for our survival. It’s not noble to suffer in silence. Fear of the world should trigger a call for help. Remaining in isolation at home runs counter to how we are wired to survive. I want to repeat this when you consider whether or not to seek treatment. In Post 18: Coping with Anxiety at Home, the final post in the series, I’ll describe coping strategies that you can do on your own. The experts say the winning combination to heal from debilitating anxiety, panic, and phobia is a combination of psychotherapy, medication, and lifestyle changes. I find that comforting to hear. We’re not our disorder, nor are we tethered to it. What we can do for ourselves is the opposite of hopeless — it’s a source of hope.