Narcissism and the Rest of Us
Show Table of Contents
INTRODUCTION
NARCISSISM DEFINED
2. Is There a Narcissist in Your Life?
3. Narcissus and the Origins of Narcissistic Thought — Part I
4. Narcissus and the Origins of Narcissistic Thought — Part II
5. Narcissus and the Origins of Narcissistic Thought — Part III
NARCISSISTIC DEFENSES
6. A Narcissist’s Self-Defense — Part I
7. A Narcissist’s Self-Defense — Part II
8. A Narcissist’s Self-Defense — Part III
NARCISSIST PERSONALITY DISORDER VS TRAITS
9. When Narcissism is a Personality Disorder
10. Narcissism and the Maladaptive Umbrella
11. Malignant Narcissism and the Narcissism Spectrum
12. When Narcissism is Compounded by Comorbidity
NURTURE VS NATURE
15. Narcissism: Flipping Self-Esteem on its Head
16. The Double-Edged Sword of Grandiose Narcissism
NARCISSISM’S DARK SIDE
19. Narcissistic Rage and Narcissistic Self-Awareness
20. Trait Narcissism and the Illusion of Control
21. Beyond Narcissism: Dark Personality Traits — Part I
22. Narcissist Sociopaths: Dark Personality Traits — Part II
ROMANTIC LOVE AND BOUNDARY-SETTING WITH A NARCISSIST
23. Romantic Love with a Narcissist — Part I
24. Romantic Love with a Narcissist — Part II
25. The Narcissist’s Non-Apology Apology
26. Boundary-Setting with Narcissists — Part I
27. Boundary-Setting with Narcissists — Part II
28. Boundary-Setting with Narcissists — Part III
29. Shattering Narcissus’ Mirror… So They Can Live
CONCLUSION
30. On Narcissism: What About the Rest of Us?
12. When Narcissism is Compounded by Comorbidity

Illustration: AI-assisted, Power of Positivity
Narcissistic personality disorder (NPD) is a debilitating condition for the narcissist and everyone around them. All aspects of life, love, and work are affected by such a serious personality disorder. So just imagine what happens when we add to it another serious mental illness or other PD, like borderline or antisocial. Everything intensifies, diagnoses and treatment regimens become more complicated—and the narcissist is further disinclined to get help because nothing improves without long-term, dedicated effort. And they know better, which of course they don’t. This is what’s meant by comorbid or co-occurring conditions. A person with one thing can commonly have another, without it being clear why.
My attempts to read scientific research papers on psychiatric comorbidity went sailing over my head, down to the mathematical (Greek?) symbols or words like the neuropsychopathological (NP) factor across externalizing and internalizing symptoms. However, I like to share my pain—the illustration above shows several graphics with how the NP factor is faring. Don’t attempt to decipher, just enjoy the colors and arrows.
What I will do in this post, however, is use everyday language to explain why comorbidity is a disaster for narcissists and for those loving, liking, coworking with, or treating them.
Narcissistic Comorbidities
It’s difficult to contend with a life-shaping disorder like NPD, but it’s often worse than that. NPD tends to be complicated by co-occurring with other mental health conditions and concerns:
- Relationship difficulties and/or problems at work or school
- Fear of vulnerability and withdrawing from others to hide this feeling
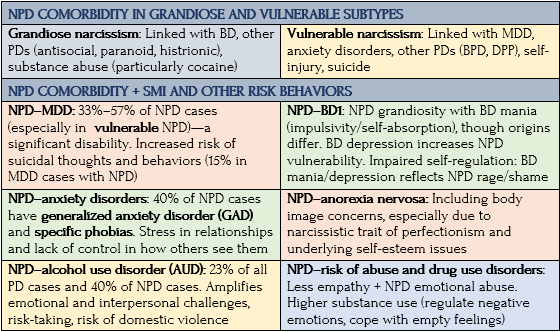
- Anxiety disorders (social anxiety, specific phobias, body dysmorphic disorder) and eating disorders (anorexia)
- Mood disorders (major depressive disorder/MDD and bipolar disorder)
- Other personality disorders, such as borderline personality disorder (BPD), antisocial personality disorder (ASPD). Also
- Physical health problems
- Substance use disorders (SUD), especially alcohol abuse when reality doesn’t meet their expectations or cocaine and other stimulant use to provide feelings they want to have
- Suicidal thoughts or behavior among those with both NPD and MDD are more likely to complete suicide.
Not a lot is known about NPD and serious mental illness (SMI). Hopefully new research will catch up, because comorbid SMIs are often the reason those with NPD seek psychiatric care. Comorbidity increases the risk of adverse outcomes, including self-harm and suicide, particularly when NPD is comorbid with BPD or ASPD. The dense comorbidity story is best told in one enormous chart:
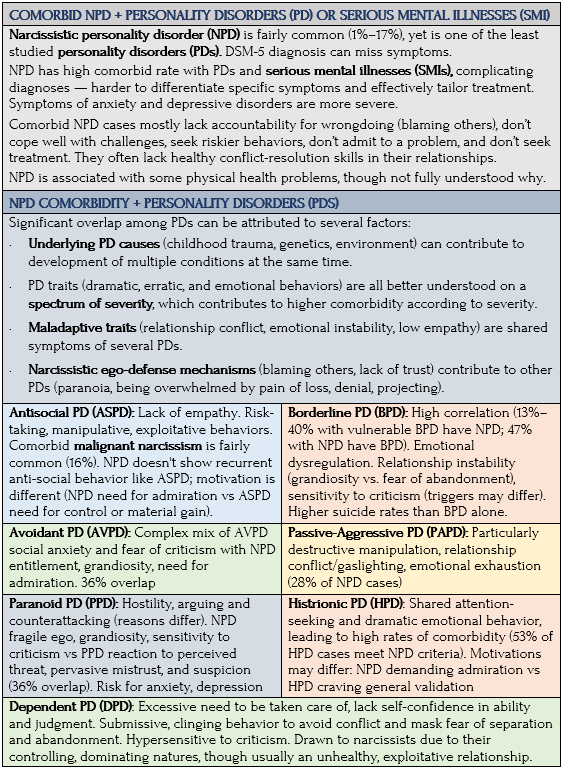
Sources: Physicians Yaakov Green and Claire Holderness, “Adding Insult to Narcissistic Injury: Comorbidity of Narcissistic Personality Disorder and Major Depressive Disorder,” Psychiatric Times; National Institute of Mental Health; Verywell Mind; Charlie Health; AMFM; AppState
A Case Study
The following case study of a middle-aged man with comorbid vulnerable narcissism and other serious mental illnesses (SMIs) is an excellent illustration of how difficult it is to treat a person who is suffering but unable to follow recommended care. The case was presented in Psychiatric Times by physicians Yaakov Green, psychiatry resident, Columbia University Irving Medical Center, and Claire Holderness, associate clinical professor of psychiatry, Columbia University Vagelos College of Physicians and Surgeons, both of NYS Psychiatric Institute. [Edited, abridged, without medical jargon/names of meds]
Jeffrey, a 52-year-old single New Yorker and former literary agent, has a history of treatment-resistant major depressive disorder (TRMDD) and generalized anxiety disorder (GAD). He was hospitalized for depression and suicidal ideation after losing his job (successful 20-year career) and partner of 15 years. He had controlled his depression and anxiety without psychiatric care, but his mental health deteriorated during COVID. He struggled to adapt to remote work and unfamiliar technology, unlike younger colleagues. His feeling of inadequacy contributed to worsening depression and anxiety.
Jeffrey “lost faith” in his healthcare when his symptoms worsened. A string of hospitalizations and various clinical trials for antidepressants, mood stabilizers, antipsychotics, ketamine, and electroconvulsive therapy (ECT) led to partial-to-no effect. His deteriorated occupational/social functioning, job and relationship losses, and worsened depression, anxiety, and hopelessness led him to plan suicide.
Admitted involuntarily to a hospital due to risk for self-harm, Jeffrey was given new drugs. Psychotherapy initially focused on his poor self-esteem and frustration, as he job searched. He tried cognitive behavioral therapy (CBT), including cognitive restructuring and exposure to new technologies.
Treatment initially helped with mood and reduced suicidal ideation, but Jeffrey was sad most days. He fixated on medication doses and adverse effects, demanding his regimen be changed. To his mother, he expressed hopelessness, frustration with his care, and feeling misunderstood by his team. He was put on a potent antidepressant that raised his energy, but didn’t improve his mood and anxiety. His team saw his anxiety coming from unrealistic expectations about how quickly his mood would improve and how easy it would be to find a job.
Jeffrey believed he’d be able to start his own literary agency and become a member of elite NYC social clubs. He envied ex-colleagues’ technological knowhow, but also criticized their inability to “read people” as well as he could. He resented their unwillingness to recognize this quality in him. In contrast, his ex-partner was an “angel,” supportive of his endeavors. He bemoaned finding another like them.
Jeffrey’s affect dramatically improved as an in-house patient, with less sleep disturbance, fatigue, concentration, and suicidality — but he still felt depressed, hopeless, and anxious. He was discharged to an acute care program. Despite frequent attendance, his depression relapsed relatively rapidly, resulting in another hospitalization.
The Vulnerable Narcissist
Jeffrey struggles with feelings of inferiority, self-doubt, and hypersensitivity, consistent with vulnerable narcissism, and depressive tendencies of poor self-definition/self-image. His grandiosity and fantasies of unlimited success and specialness — with unique interpersonal skills, special talents at work, unconditional admiration in personal relationships — are narcissistic defenses to protect this fragile self-image.
Stressors (job loss/breakup) can inflict narcissistic injuries—perceived threats to self-esteem—overwhelming his defenses, causing withdrawal, depression, self-accusation. He’s embarrassed and disappointed, envious of others, and feels misunderstood, mistreated, and powerless. His dependent character structure (over relying on his treatment team, needing his mother’s constant reassurance) reflects his self-doubt.
Jeffrey’s condition is consistent with research on the comorbidity of vulnerable narcissism and dependent personality disorder (DPD). His rapid affective changes reflect responses to treatment as well as his vacillating self-esteem.
Medication helps with Jeffrey’s depressive symptoms (sleep disturbance, decreased energy, poor concentration), but fail to sufficiently treat the guilt, worthlessness, social withdrawal, and depressed mood that reflects his underlying personality dysfunction.
His care is fragmented as he seeks new treatment teams, often oscillating between overdependence and devaluation. Jeffrey is therefore unable to engage in possibly the most effective treatment for him: a consistent psychopharmacologic regimen targeting symptoms, in combination with long-term, evidence-based psychotherapy.
Clinical Challenges
Jeffrey’s case shows the challenges in diagnosing MDD in individuals with NPD’s vulnerable traits. Overlapping symptoms make it difficult to attribute symptoms to the mood disorder or to the character pathology. There are also challenges with psychotherapy. Narcissists with exaggerated self-esteem don’t always recognize their problems and engage in treatment. The therapeutic alliance is challenged by therapists feeling coerced to find a panacea or feeling disparaged as incompetent.
Although treatment guidelines are scant, many of the recommended therapeutic approaches — mentalization-based therapy, transference-focused psychotherapy, schema-focused psychotherapy, and dialectical behavioral therapy — are adapted from the treatment of borderline personality disorder (BPD).
Treatment success requires a long-term relationship between patient and therapist, which is impractical in acute care. It’s not surprising that Jeffrey, with comorbid NPD and major depression, has a slower and less significant recovery.
Another difficulty is in identifying NPD when the prominent traits are not externally conspicuous behavior, but vulnerability. In terms of long-term psychotherapy, what’s needed is nonjudgmental, curious interventions that use the patient’s own words and recognize their vulnerability, ultimately challenging their self-criticism and encouraging interpersonal connections. Therapy should also set clear and achievable goals that are periodically reviewed with the patient.
Concluding Thoughts
NPD and MDD are common, and commonly comorbid, disorders, causing a significant level of distress and dysfunction. While individuals with NPD don’t often seek care, a major depressive episode may bring them to clinical attention, necessitating diagnosis and appropriate treatment of both conditions. Although the co-occurrence of NPD and MDD may add insult to injury for patients and compound challenges for clinicians, appropriately recognizing and addressing both may soften the blow. —Yaakov Green and Claire Holderness, “Adding Insult to Narcissistic Injury: Comorbidity of Narcissistic Personality Disorder and Major Depressive Disorder,” Psychiatric Times
Coming Up Next

The 21st century is about moving from theory to science — from surmising what causes narcissism to discovering its origins, using modern scanning technology and normed, validated questionnaires across large populations of people. In this way, another picture of narcissism emerges. It won’t be too surprising to learn the personality disorder — that is, narcissism in its most pronounced form — is the result of a multitude of factors: environmental (nurture) and genetic and neurobiological (nature). In Post 13: The Nurture of Narcissism, I give examples of research, without trying to be comprehensive. My aim is not to write a book, but to impart some idea of how little we yet know and the promise for the future.