On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
1. On Bipolar Disorder: Introduction

Photo © Oliver Rossi | Getty Images
I’m writing this series on bipolar disorder because my older son Jaden lives with bipolar I. What began as a personal effort to understand his illness gradually turned into a deep look into the science of bipolar disorder — a condition affecting roughly six million people in the United States and tens of millions worldwide. I hope to provide information and support for anyone diagnosed with bipolar disorder (BD), suspecting they have BD, or caring about someone with BD — like I do.
I didn’t set out to write about the impact of neurons, genes, and the brain on mental illness — but it’s impossible to understand this lifelong mental illness without this grounding.
Bipolar is often described as a mood disorder, because mood changes are the most visible part of it. But researchers increasingly understand it as involving several biological systems, including reward sensitivity, circadian rhythm, stress regulation, and emotional amplification — all topics I will touch on in this series.
I hope the ultimate message will be how BP symptoms can be managed in this chronic, lifelong condition, knowing it can be a daily struggle.
I’ll talk about BD and tell my 37-year-old son Jaden’s story, hopefully from both our perspectives — as he’s agreed in principle to contribute. This may be the first time he talks “on the record” about his 13-year-and-counting odyssey with bipolar I (BD-I). His story is hard to tell in places because it has an unrelenting character — it doesn’t improve with maturity, but maturity helps to manage it so life is worth living.
Brief History of Bipolar Disorder
What we now call bipolar disorder was once known as manic depression and, long before that, it was simply observed as a recurring pattern of human suffering. According to historical accounts summarized by sources such as Wikipedia, descriptions of extreme mood states stretch back thousands of years.
The terms melancholia (deep sadness) and mania (agitation or frenzy) come from Ancient Greek medicine. Physicians as early as Hippocrates believed these states were rooted in bodily processes rather than moral or spiritual failings — a remarkably modern idea. Medical writings from first-century Greece describe the use of mineral salts to calm people experiencing extreme mood disturbances. Notably, some of these salts contained lithium.
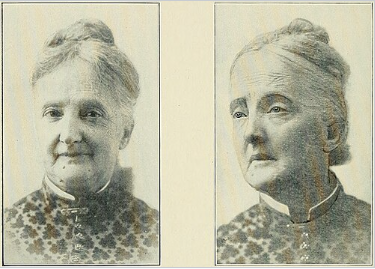
Woman with folie circulaire (circular insanity), showing manic (left) and depressed (right) states, Wikipedia
That detail feels almost uncanny from a modern perspective. Today, lithium — still derived from mineral salts — remains one of the most effective and enduring BD treatments.
In the mid-19th century, French psychiatrist Jean-Pierre Falret took a major step toward formal recognition of the condition. In 1851, he described folie circulaire (circular insanity) — a pattern of alternating mania and depression with periods of relative stability in between.
At the turn of the 20th-century, German psychiatrist Emil Kraepelin emphasized the biological basis of mental illness and observed how symptoms unfolded over time.
He distinguished manic-depressive illness from schizophrenia, arguing that mood disorders followed a cyclical course rather than a progressively deteriorating one. His diagnostic framework — grounded in long-term patterns rather than isolated symptoms — still influences psychiatric classification today.
From ancient mineral baths to modern mood stabilizers, from poetic descriptions of melancholy to systematic clinical observation, BD has always been with us.
What has changed is not the condition itself, but our willingness to see it clearly — and to treat it as an illness rather than a personal failing.
Today, lithium — still derived from mineral salts — remains one of the most effective and enduring treatments for bipolar disorder, first introduced into modern psychiatry in 1949.
Emil Kraepelin, first to distinguish bipolar disorder from schizophrenia, Wikipedia

Bipolar “Spectra” and Prevalence
Bipolar disorder (BD) exists on not just one, but many spectra (plural of spectrum). The mental health field is increasingly aware of the significance of seeing physical and mental illness this way. Not just the traditional way — a single spectrum, usually from bad to worse — but also as co-occurring (comorbid) spectrum with other disorders that share genetic traits and environmental stressors. They look at how comorbidity doesn’t just pile up symptoms like stacking blocks, but makes symptoms worse, treatment harder, prognosis less bright. This is the story of bipolar spectrum disorders (BSD) on multiple fronts.
Evidence supports the idea that “many mental disorders lie on a spectrum, or series of spectra, linked by shared genetics.” —British journal Psychiatria Danubina
In the case of BD, multiple spectra frame our understanding of the complex permutations of this illness and the ways those living with it can find a path through accompanying pain and loss. The first spectrum is traditional, looking within a single disorder. The second, called the bipolar spectrum, recognizes subthreshold bipolar conditions and the frequent overlap between bipolar disorder and other psychiatric disorders.
Traditional Bipolar Spectrum
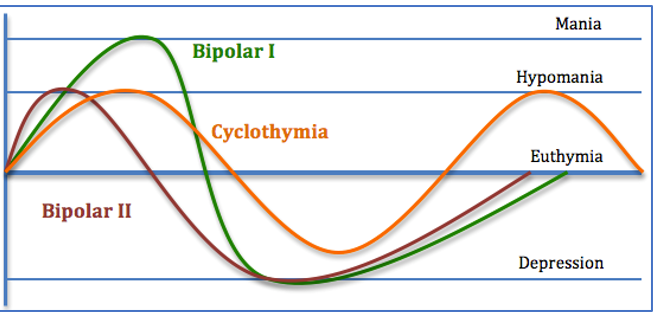
Graphic: Wikipedia illustrations
The typical spectrum — like autistic spectrum disorder (ASD) — is focused on severity within one classified disorder. In the case of bipolar disorder, this spectrum is excellent health at one end to cyclothymia to bipolar II to bipolar I — the latter carrying the most debilitating symptoms — at the other end. This is the approach taken by the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders or DSM-5 guidelines. It looks across a range of:
- Alternating episodes of mania/hypomania and depression
- Severity and frequency of cycles and symptoms
- Ways of coping, getting better, and maintaining a healthy regimen
- And, increasingly, at sleep-wake cycles (circadian rhythm), stress regulation, and reward sensitization — all these topics will be covered in this series.
Bipolar Spectrum Conditions
Increasingly prominent is a newer designation of bipolar spectrum conditions. According to WebMD, the bipolar spectrum shows the “family relationship” of overlapping conditions, with some shared genetics and symptoms — not suggesting one caused the other, but suggesting a correlation.
BD shares some genetic traits and behavioral symptoms with many serious mental health disorders and conditions, including:
- Impulse control disorder, like conduct disorder (CD)
- Attention-deficit/hyperactivity disorder (ADHD)
- Anxiety disorders and other mood disorders, like major depressive disorder (MDD)
- Personality disorders (PDs), like borderline personality disorder (BPD)
- Substance use disorder (SUD)
Some spectrum conditions can involve other mood disorders or trait conditions with ups and downs, but without manic or hypomanic episodes. There can also be comorbid conditions with physical health conditions, like cardiovascular disease [see post 21 on new research].
“Overlaps” Among Multiple Bipolar Spectra
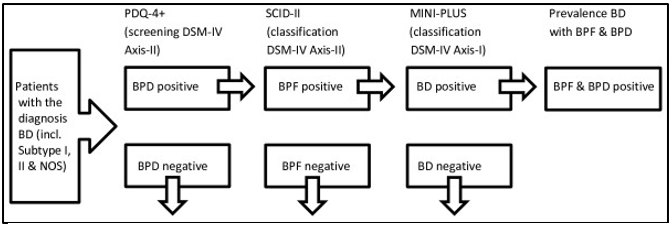
Illustration: ResearchGate
This way of looking at BD is not just intellectual speculation. Understanding how correlations compromise treatment leads to improved treatment outcomes — so individuals can get on with their lives. Mental health specialists need to consider both the parameters of a single disorder, as described in DSM-5, and the constellation of disorders that show up in a single individual.
Mental health researchers and experts are proposing “no absolute cut-offs to diagnoses and treatments of mental health disorders and conditions, but rather an emphasis on the impact the problems are having on patient functioning.”—Psychiatria Danubina
Bipolar Prevalence in the General Population
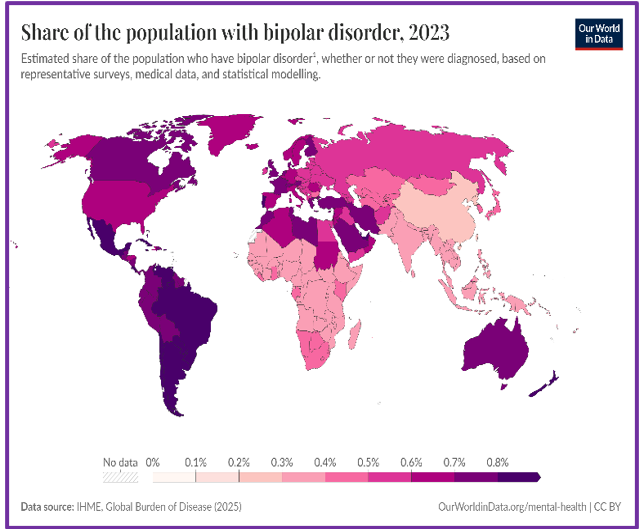
Graphic: Our World in Data
Bipolar is a complex mood disorder that disrupts a person’s life and affects their parents, siblings, friends, spouses or partners, work colleagues, and schoolmates. It turns out BD is fairly common in the U.S. and around the world.
Research is from the National Institute of Mental Health (NIMH) or NIMH’s citing of diagnostic interview data from National Comorbidity Survey Replication (NCS-R), unless otherwise noted.
More Common Than many other conditions
BD is considered one of the leading causes of disability worldwide (World Health Organization):
- About 4.4% of U.S. adults experience BD at some time in their lives.
In any given year, BD affects:
- Almost 3% of the U.S. adult population, translating to nearly 6 million people
- About 2% globally, translating to roughly 40–50 million people
- Men (2.9%) and women (2.8%) near equally
- People in every race, ethnic group, and social class
High Risks to the Lives, Livelihoods, and Physical Medical Health
Fully 1/3 of people with BD have financial, social, or work-related problems — a huge cost to the individuals themselves, their families, and society.
Due to unhealthy lifestyles, misdiagnoses, and medication side effects in people with BD:
- Risk of death from natural causes (like heart disease): two times higher than general population
- Results in 9.2 years less than average expected life span
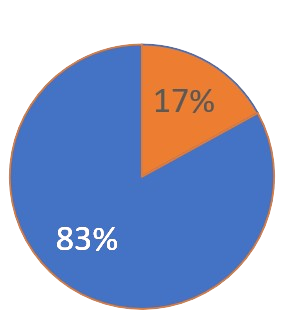
Bipolar Disorder Impairment Among Adults
In the past year, the estimated degree of impairment ranged from moderate to serious among those with BD, as follows:
- 83% of people had serious BD impairment — the highest percentage of serious impairment among mood disorders.
- 17% had moderate impairment.
High risk of suicide and self-harm among those with BD:
- Persons with BD are 12 times more likely to commit suicide than the general population.
- 25%–60% attempt suicide at least once in their lives; 4%–19% die by suicide.
- Another 30%–40% engage in self-harm.
Graphic: Jan Swan
Late Adolescence — Early Adulthood: Peak Years for BD Onset
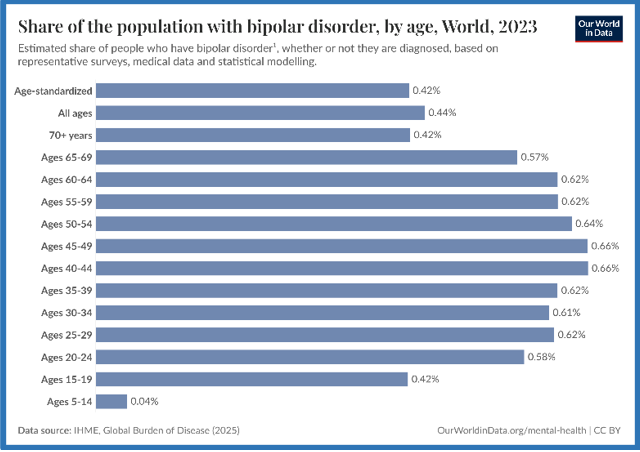
Graphic: Our World in Data
2/3 of adults with BD have at least 1 close relative with BD or unipolar depression (that is, major depressive disorder/MDD). This indicate BD is a partially inherited condition.
- Symptoms commonly begin by ages 20-25 — though can start in early childhood or as late as the 40s-50s.
- The earlier the onset the worse the prognosis.
- Among adolescents, prevalence higher for females (3.3%) than males (2.6%)
Women with BD II
- More likely than men with BD II to experience rapid cycling periods (Psychological Medicine)
- More depressive and more mixed episodes (Journal of Clinical Psychiatry)
Children and Adolescents

Photo: Instagram
- BD is more likely to affect children of parents with BD: the risk to the child of 1 parent with BD is 15%-30%, but the risk with 2 parents with BD is 50%-75%.
May be as common among youth as adults. 1% of teens (ages 14-18) met the criteria for BD or cyclothymia in their lifetime.
20% of adolescents with MDD develop BD within 5 years of depression onset (Childhood and Adolescent Depression).
- 1/3 of 3.4 million U.S. children and adolescents with depression may be experiencing early BP onset (American Academy of Child and Adolescent Psychiatry, 1997).
- In contrast to adults, manic children and adolescents are more irritable and prone to destructive outbursts than to be elated or euphoric.
- Depression may show up as physical complaints (headaches, stomachaches, tiredness), poor performance in school, irritability, social isolation, and/or extreme sensitivity to rejection or failure (National Institute of Mental Health).
BD in Young Adults (Ages 18-30)
Transition to adulthood is challenging for most young people — gaining financial independence, finding jobs, schooling, relationships — but it’s especially tough for those with mood disorders.
BD in older adults
Uncommon to appear for first time in late life, but some may have symptoms throughout their lives but are only diagnosed later.
Older adults have more medical problems and take more medications — their comorbidities need to be considered in managing their BD.

Photo: Alamy
Comorbidity
Here’s what we know about the prevalence of co-occurring psychiatric disorders, according to studies cited by the Cleveland Clinic and other sources:
- More than 60% of people with BD have at least one additional psychiatric diagnosis, most commonly anxiety disorders, substance use disorder, ADHD, or personality disorders.
- According to DSM-5, an individual may be diagnosed with both BD and narcissistic personality order (NPD) only if grandiosity observed during a manic episode remains present when individual is euthymic (calm mental state between cycles) and a personality disorder (PD) can’t be diagnosed during an untreated mood episode.
- Comorbidity studies find “cluster B” PDs — NPD, borderline personality disorder (BPD), antisocial personality disorder (ASPD), and histrionic personality disorder (HPD) — are the most common among BD patients euthymic at time of testing and among hospitalized BD inpatients.
- NPD was diagnosed in 4.5%–8.3% of these patients, which is a higher rate than 0%–6.2% community prevalence rate in DSM-5.
- Connections between BD and NPD have emerged in other studies. Diagnosis with a comorbid PD predicted a worse overall course of symptoms among BD inpatients, even when in remission.
A Few Notes
In post 2, I’ll start Jaden’s story, renewing some painful history through the lens of bipolar spectrum disorders (BSD) and how it affects his daily life and threats to his future. Jaden, now 37, was diagnosed with ADHD as a child and a severe BD type as a young adult — but he’s also suffered from anxiety, trauma/PTSD, and perhaps a personality disorder. Some would say his cannabis use is an addiction, but too much is unclear about that.
I will also reflect on the impact of his illness on me — his mother, emotional rollercoaster person, support team, and fan club treasurer. Although I have no training or expertise in healthcare or mental health, I consider myself an amateur science reporter on mental health topics.
Image: ATA Scientific
Time to time, I express my outrage and sense of powerlessness about how little help there is for those struggling with mental illness.
Hopefully, this helps us proactively seek out our own care or support someone we love with theirs, even if only emotional support. This is no whitewash. My son’s life has been hard. I do what I can to alleviate some of his pain, but the burden of supporting him financially has taken a toll on me — and our relationship.
Coming Up Next

Unlike the many excellent professionals and resources available, I’m not in the advice-giving business. These posts are meant to inform, certainly, but also to support you or help you to support another in managing symptoms and fighting to live a long, rich life — not in the shadows but in full sunlight. In the next two posts — Post 2: Jaden’s Story: A Journey to Mania, and Post 3: The Bipolar Rockies: A Witness to Mania — I share in detail Jaden’s childhood experiences up through his first manic/psychotic episode, a year before he’s “officially” diagnosed with bipolar disorder.