On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
13. Bipolar Spectrum: Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
Correct diagnosis of illness is the foundation of effective treatment. But for many people with bipolar disorder, that diagnosis comes far too late — if it comes at all. Bipolar is one of the most studied and treatable psychiatric conditions. Yet in practice it’s frequently missed, mistaken for other illnesses, or recognized only after years of disruption. Many people live through multiple mood episodes before the pattern becomes clear. Others receive treatment for depression alone, unaware that their depressive episodes are only one side of a larger mood cycle.
This delay is not simply a clinical problem. It’s also a social one.
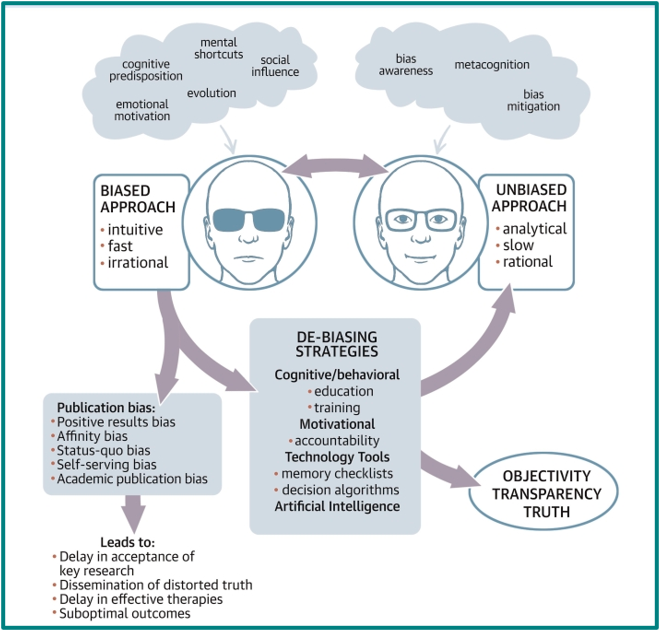
Source: M. Elizabeth Hammond, MD, “Bias in Medicine: Lessons Learned and Mitigation Strategies, Science Direct

Why Bipolar Disorder Carries So Much Stigma
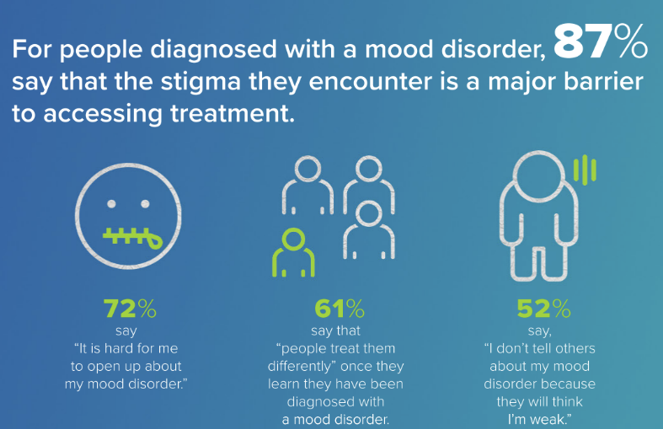
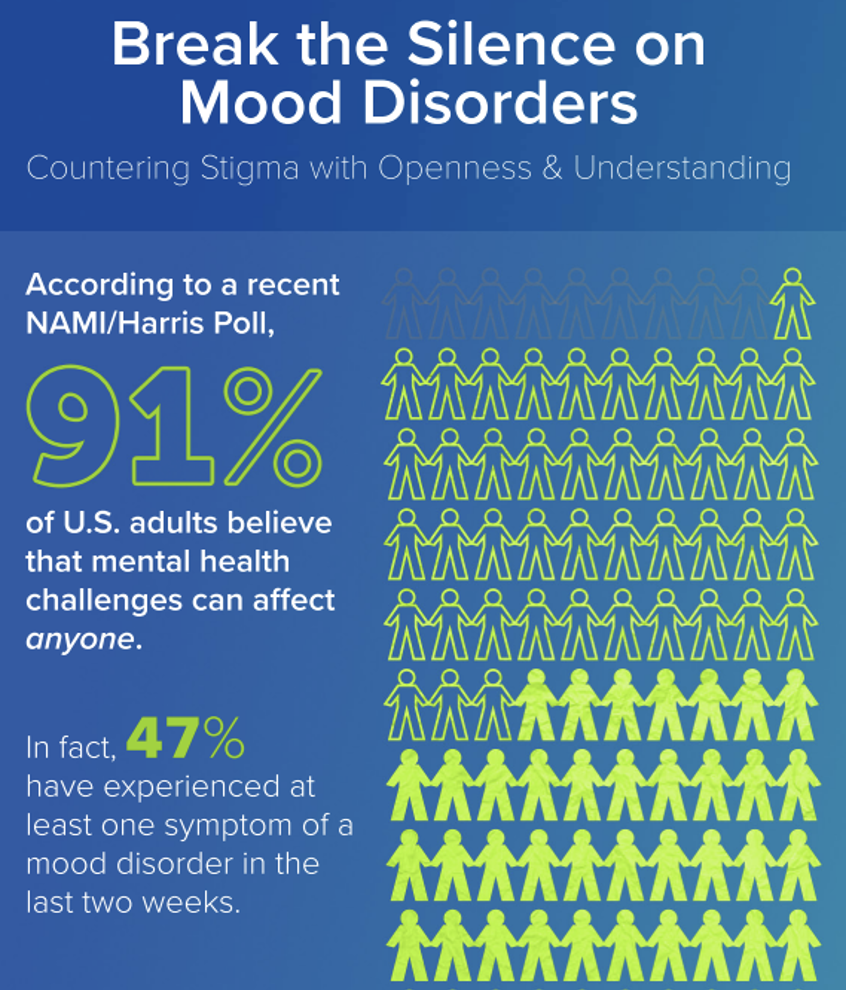
Research consistently shows bipolar disorder is widely misunderstood and heavily stigmatized. According to the 2021 National Alliance on Mental Illness (NAMI), stigma remains one of the major barriers preventing people with mood disorders from seeking care. In a national survey, 87% of Americans said stigma was a major obstacle to treatment. And many individuals with mood disorders reported feeling judged, misunderstood, or treated differently after others learned about their diagnosis.
These misconceptions are persistent, and they feed stigma. The NAMI survey also found large numbers of Americans believe BD is simply a more severe form of depression, while others see it as a flawed or weak personality rather than a medical condition. In public attitude surveys, respondents reported feeling uncomfortable around someone with BD or believed that people with the illness were fundamentally different from others.
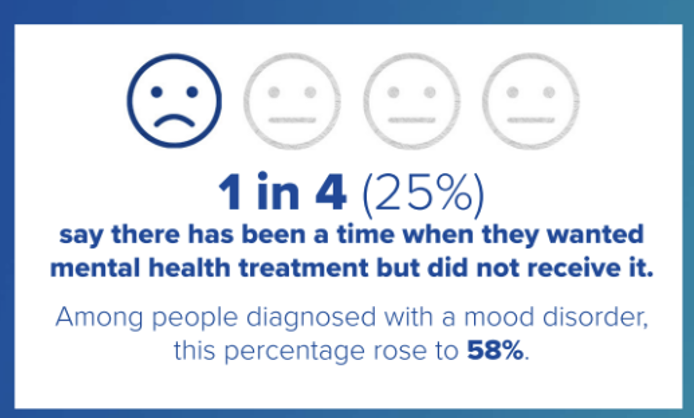
Even when people want help, the fear of being labeled can silence them. Stigma can stop treatment before it begins. This is particularly true for younger adults. In one survey, 38% of young adults who went without mental-health care said fear of judgment kept them from seeking help.
When people fear the label of bipolar disorder more than the symptoms themselves, they often delay seeking help — or avoid describing the very experiences that would make the diagnosis visible.
Stigma, Pain, and Suffering
The ubiquity of these forms of prejudice and stigma can be devastating for the roughly 40 million worldwide Th with bipolar disorder — even though it isn’t a particularly rare condition.
To put that number in perspective, consider three neurological diseases widely recognized as serious medical conditions evoking sympathy, medical urgency, and coordinated care: multiple sclerosis, Parkinson’s disease, and amyotrophic lateral sclerosis (ALS). Together, those illnesses affect upward of 14 million people globally — far fewer than half the number of people living with bipolar disorder.
Yet the public response to these conditions often looks very different. Behind these numbers are millions of individuals and families navigating an illness that is medically complex, often misdiagnosed or diagnosed late, and socially misunderstood.
The Language of Labels
Mental illnesses are often misunderstood, but bipolar disorder occupies a particularly difficult place in the public imagination.
Part of the problem is language. In everyday conversation, the term bipolar is used casually to describe ordinary moodiness or unpredictability. This trivializes the illness while also reinforcing the stereotype that people with BD are unstable, unpredictable, or dangerous — certainly incapable of functioning like “normal” people. Another is the unfortunate use of a label beginning with “bi,” which overly reduces the disorder to happy/sad faces like theater masks for drama and comedy — a wholly inadequate reflection of its nature.
I generally prefer mental health condition to mental illness for this very reason. Yet, I write mental illness when describing activated symptoms for a serious condition.
Just not to describe a person (people are not their condition). No one is bipolar. They have bipolar. This is what’s meant by “people-first” language.
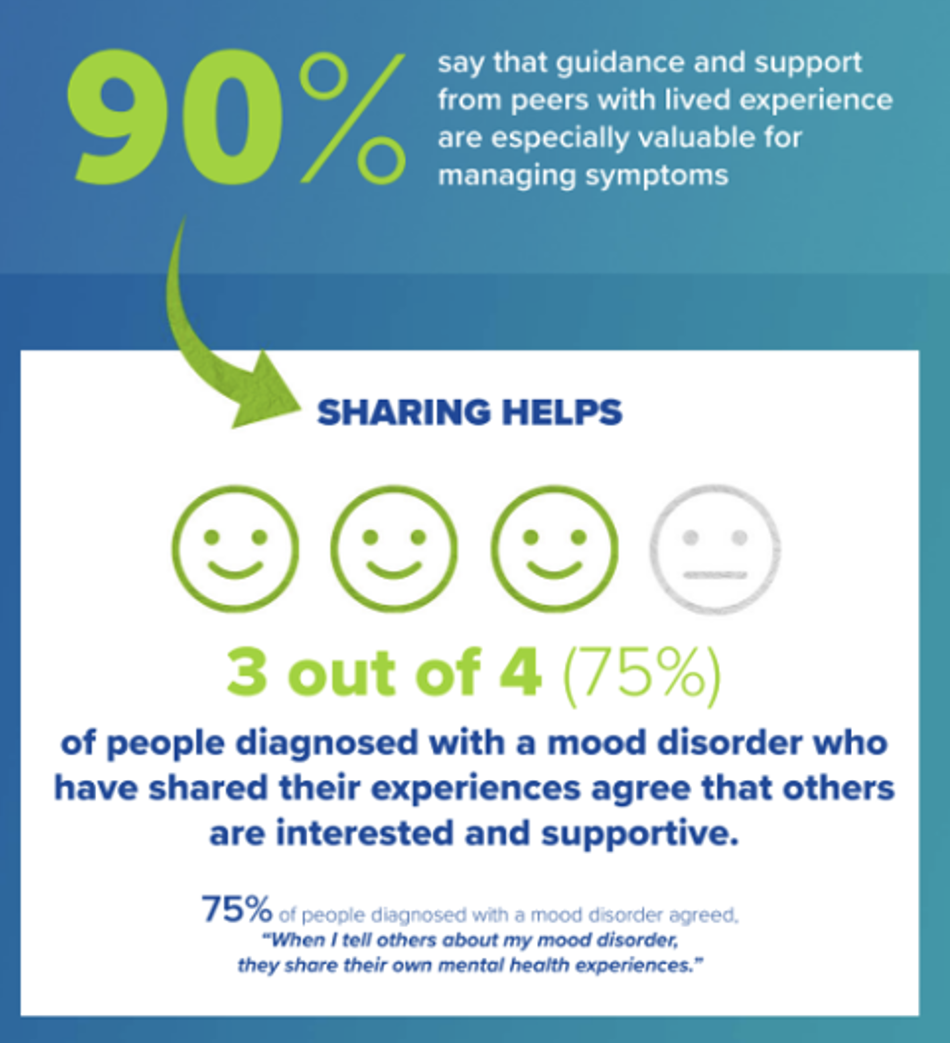
A majority of people with mood disorders say they are treated differently once others know about their diagnosis, and many report that friends, coworkers, or even family members struggle to understand what the illness is actually like. For those living with the condition, the impact can be deeply personal, as frien,ds and family give them wide berth.
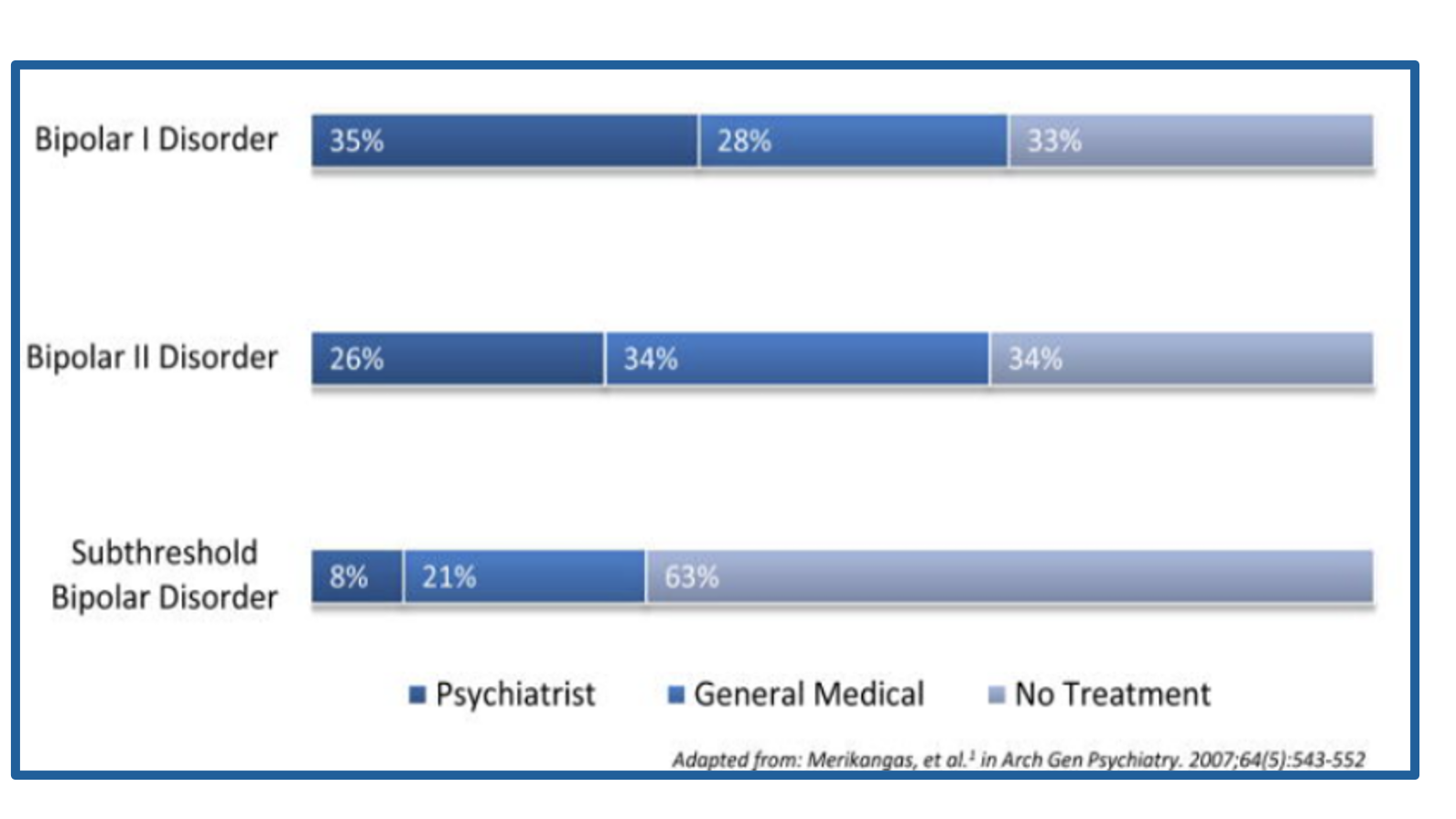
In the past 12 months, proportion of individuals with bipolar I, bipolar II, or subthreshold bipolar disorders receiving treatment from a psychiatrist, general medical clinic, general medical clinician, or no treatment. From Joseph Cerimele, “Bipolar Disorder and Population Health,” PubMed Central/NIH
Over time, these social pressures can become internalized. Research synthesized by Joseph Cerimele, “Bipolar Disorder and Population Health,” PubMed Central/NIH, shows people with BD often experience internalized stigma — absorbing negative beliefs about their illness and applying them to themselves. Since many already struggle with self-esteem and self-worth during mood episodes, this can exacerbate feelings of shame and perpetuate secrecy and reluctance to seek help.
And while it deserves a lot more attention than I will give in this series, racial and cultural prejudices follow people into the doctor’s office. It’s an appalling reality, which doesn’t go unnoticed. Not only that, but surveys of psychiatric professionals — still largely white — show prejudicial treatment of people of
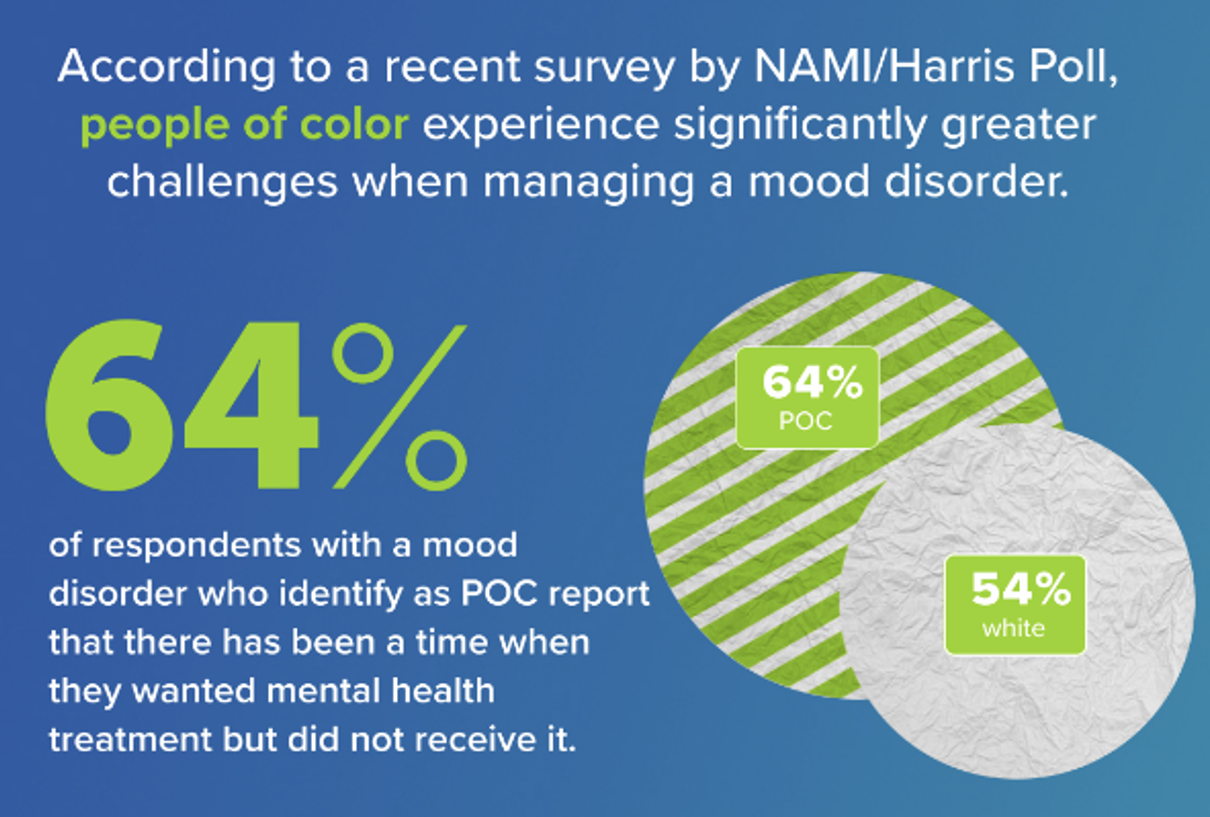
color. Finding, for example, a Black male psychologist to treat perhaps your Black son is not an easy task. It’s not to say you must “match,” but it does help to find someone who understands how racial stigma sits on top of mental health stigma.
If I sound like I’m pounding the table, it’s because I am. I’ve watched up-close what stigma can do to a vulnerable person navigating bipolar disorder — encountering misunderstanding not only from family and friends, but sometimes from medical professionals, government bureaucracies, and social services that leave people to fend for themselves when they are least able to do so.
The Consequences of Silence
The main reason stigma directly interferes with timely diagnosis and treatment is because people with troubling symptoms hesitate to talk openly — especially when it comes to mania or hypomania. Elevated mood, bursts of energy, racing thoughts, or periods of intense productivity may not feel like illness at all. In fact, they can appear like the most creative or successful moments in a person’s life. Viewing their experiences through a stigmatizing lens may cause them to avoid doing anything that leads to an undesired label.
Depression, on the other hand, is more widely recognized and socially accepted. People are far more likely to seek help when they are struggling with low mood, exhaustion, or hopelessness. Not only that, clinicians seeing no clear evidence of mania/hypomania may mistake BD as major depressive disorder (MDD).
The result may be years of potentially treating the wrong psychiatric condition which can worsen the very condition they’re attempting to treat.
In the prior post, I discussed how treating depression with antidepressants can actually trigger manic episodes. Stigma in this instance contributes to the wrong treatment because neither doctor nor patient was clear about symptoms, onset, rhythms, and energy. Hiding the illness from professionals sets a person on the path to an inaccurate diagnosis — with far more suffering than should be.
A Way Forward
A good sign is the trend is moving toward greater awareness and destigmatizing of bipolar disorder — bipolar medications are now advertised on TV— along with more medical attention to the consequences of overlapping traits and comorbidities that confound diagnoses.
What will hopefully follow is even more effort to reduce stigma and prejudice. And more people paying attention to their own or their loved one’s symptoms and patterns — not just mood, but energy, persistence, duration, behavior, and outlook.
Adults with bipolar also need to be active consumers of their own care, from diagnosis through treatment — but only if their voices can be heard by the medical establishment and their needs for serious resources be addressed by government funding.
Stigma does not only shape public attitudes. It also shapes how people understand themselves — and the labels they receive.
Meet Darren: The Word That Felt Worse Than Bipolar

Darren looks younger than his 41 years. A former college soccer coach and adjunct English instructor, he now freelances as an editor and writer. It’s unsteady, financially precarious, but it allows him to work from home and step off the “career” treadmill. He lives with Katie, his long-term partner, is estranged from his one sibling, and both parents are gone.
But now Dareen looks more tired than athletic: glasses, casual clothes, a posture that alternates between self-assured and withdrawn. In photos, he often appears dazed, not smiling, gaze slightly averted.
Photo: iStock
He was diagnosed with bipolar disorder I after a particularly upsetting incident where he shoved Katie away from him, got in his car, and drove recklessly down the street until he was pulled over and taken to a psychiatric facility. Luckily, he was disoriented enough that authorities intervened and prevented something worse from happening.
Medication brought him back to safety with some assurance of stability. The diagnosis was devastating but clarifying. It explained years of uneasy behavior and fighting with his girlfriend.
As a white male jock who snapped towels with the best of them, Darren was ashamed of his diagnosis, which he felt weakened his persona. He knew the locker room culture would chew him up and spit him out. While he worked hard to accept his newly labeled condition — as a brain illness, not a moral failing — he was also shedding friends and becoming increasingly isolated in fear of what he might do in public. He often didn’t leave his house for days at a time.
Years into treatment, Darren’s therapist raised the possibility of narcissistic traits — pointing to patterns of defensiveness, entitlement under stress, intense needs for validation, and Katie’s accusation of being empathy-deprived.
The word lands like an accusation, however. For Darren, bipolar was all the stigma he could handle. And now he’s a narcissist? It felt annihilating. He wonders whether he’s just a terrible and terribly flawed human being and wouldn’t blame Katie for leaving him. To Darren, “narcissist” isn’t a clinical term — it’s a moral verdict. He spirals: Was my suffering just self-absorption? Was my pain fake? He fears telling anyone. He briefly considers quitting therapy.
Luckily Darren works through his self-pitying denial more quickly and takes time to educate himself. He’s fairly sure he’s not narcissistic, but his mania — even though more controlled by medication — leads him to exhibit a self-confidence and somewhat grandiose persona that can resemble narcissism. What no one has told him is that his traits are shaped by vulnerability, and mood instability isn’t the same as a fixed personality disorder.
At the same time, when he ventures to explain to Katie all that’s bothering him, he’s surprised by how loving and supportive she is. She quietly suggests he get in touch with some old teammates and start making a life for himself outside their home.
Darren learns not to get bogged down by labels, but to understand how he can view his varying mood and personal behaviors as a part of him, not as verdicts on his character. To see them as odd patterns — some episodic, some enduring — that are responsive to understanding and care. He also vows to get a job teaching English as a second language, with steady income, health benefits, but low pressure.
Only when he begins to integrate the idea of his mental illness without annihilating his self-worth does he see a brighter future.
Darren’s story also highlights another challenge: diagnosing bipolar disorder is rarely straightforward. Even when clinicians recognize that something is wrong, distinguishing bipolar disorder from other conditions requires careful assessment.
Bipolar Diagnosis: As Complicated as the Symptoms?
Earlier posts covered bipolar’s highly disruptive mood episodes. But subsequent posts took a deeper look at bipolar’s neurobiology — what a stressed system looks like before overt symptoms even show up. What researchers sometimes call a hypomanic personality — a temperament marked by high energy, ambition, and reward sensitivity — can signal increased vulnerability to the disorder because of this underlying biology [see post 10 on reward sensitivity]. This means, in addition to a degree of heritability, that their body systems are already highly sensitized to the effects of cumulative stress, dysregulated circadian rhythms, and misaligned energy.
Understanding bipolar this way has been the subject of research for two decades — but this approach to assessing the disorder is still uncommon in clinical practice. It remains little understood by individuals experiencing signs that something isn’t right, as well as by doctors and families. It’s often only when the first mood episodes appear and routines are compromised that diagnostic explanations are sought — but early signs were there.
Admittedly, it’s difficult to notice these signs. Because of this, diagnoses are delayed. The implication is the need to pay more attention to so-called prodromal traits that precede a full manifestation of the illness — a challenging task for everyone involved.
Because bipolar disorder can resemble several other conditions, a careful diagnostic evaluation — often by a psychiatrist or clinical psychologist, along with a medical assessment — is usually recommended. But it’s a long road to get to a correct diagnosis.
Seen in this light, bipolar disorder begins to look less like a condition defined only by swings in mood, and more like a disorder of interconnected systems — shaping sleep, stress, energy, and even physical health over time. This broader understanding is still emerging, and the language we use has not fully caught up. The name suggests two emotional poles, but the reality is more complex, more systemic, and often more hidden. For someone receiving a diagnosis, this gap between the name and the lived experience can be disorienting. It is often not just the diagnosis itself that shocks — but what it seems to mean, and what it leaves unexplained.
More on Family History
Bipolarity runs in families, so someone is at increased risk if there’s a family member who has been diagnosed with any mental illness. As research targets BD genetics, mental health specialists are paying more attention to family history. According to psychiatrist Andrew Cutler, interviewed on a podcast for Psychiatric Times, BD is “highly genetic” and “more genetically loaded than unipolar depression.” He explains the risk starkly:
It’s helpful clinically to dig hard for a family history of mood disorders. If you get a family history of bipolar disorder or manic depression, that’s very fortunate, but we don’t always get that exact terminology…. I will ask about recurrent mood episodes, any family members that had depression or mood episodes, substance abuse, and family history of suicide. Because patients with unipolar depression attempt suicide, but patients with bipolar commit suicide. They tend to use more lethal attempts.
Medical and mental healthcare specialists need to ask people some tough questions — and hopefully they receive detailed answers — including whether anyone in the family has:
- Attempted or died by suicide
- Had electroconvulsive shock therapy (ECT)
- Been involuntarily committed to a psychiatric hospital
Misdiagnosing Bipolar Disorder
BD misdiagnosis causes people with the disorder to suffer longer, and their prognoses worsen as a result. Early detection for genetic illnesses is crucial, yet people with BD often wait years before receiving the correct medication, therapy, and strategies needed to stabilize their lives.
For most people with BD, their depression lasts much longer than mania/hypomania, making it more likely they’ll seek help when depressed. Without mania being observed or reported, healthcare specialists can easily mistake BD for unipolar major depressive disorder (MDD).
Clinicians diagnose BD by identifying patterns of mood episodes over time, including periods of mania, hypomania, and depression. But research shows it can take 5–10 years between the onset of symptoms and an accurate diagnosis.
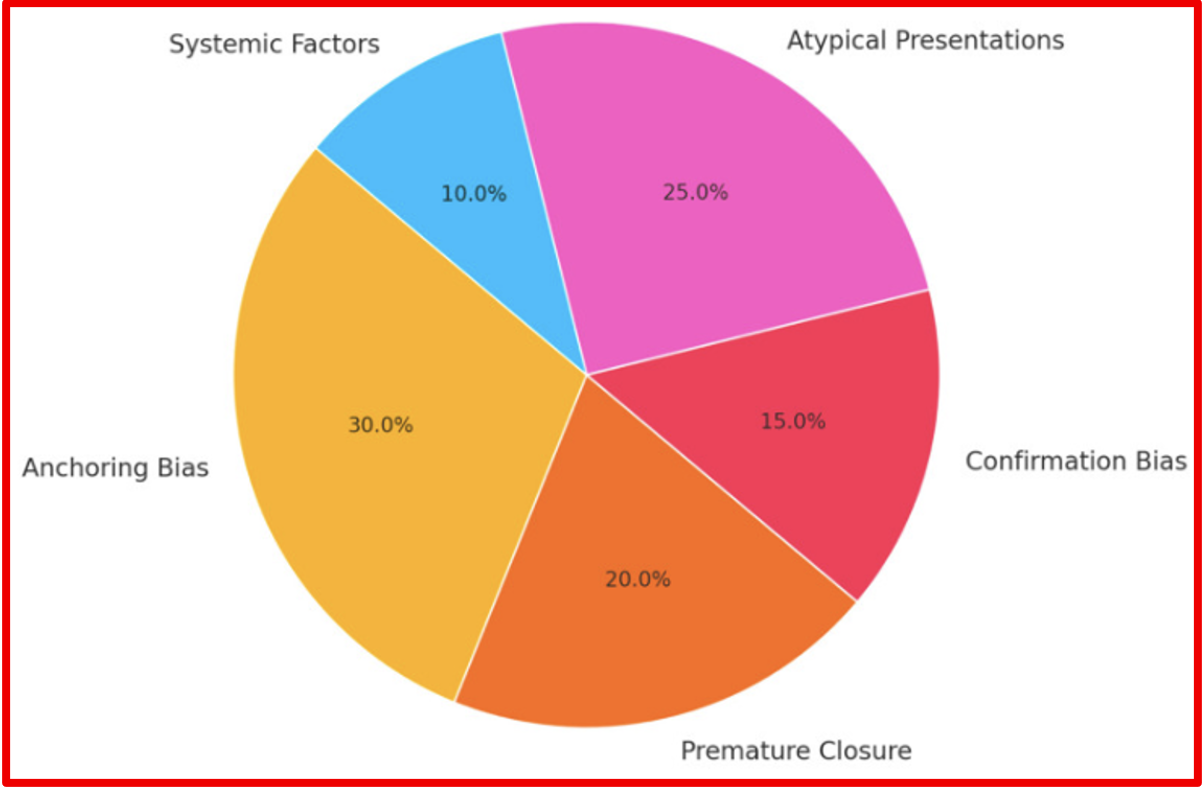
Proportional distribution of diagnostic errors, from: Zeinab Mutlak, et al., “The Misdiagnosis Tracker: Enhancing Diagnostic Reasoning Through Cognitive Bias Awareness and Error Analysis,” PubMed Central/NIH
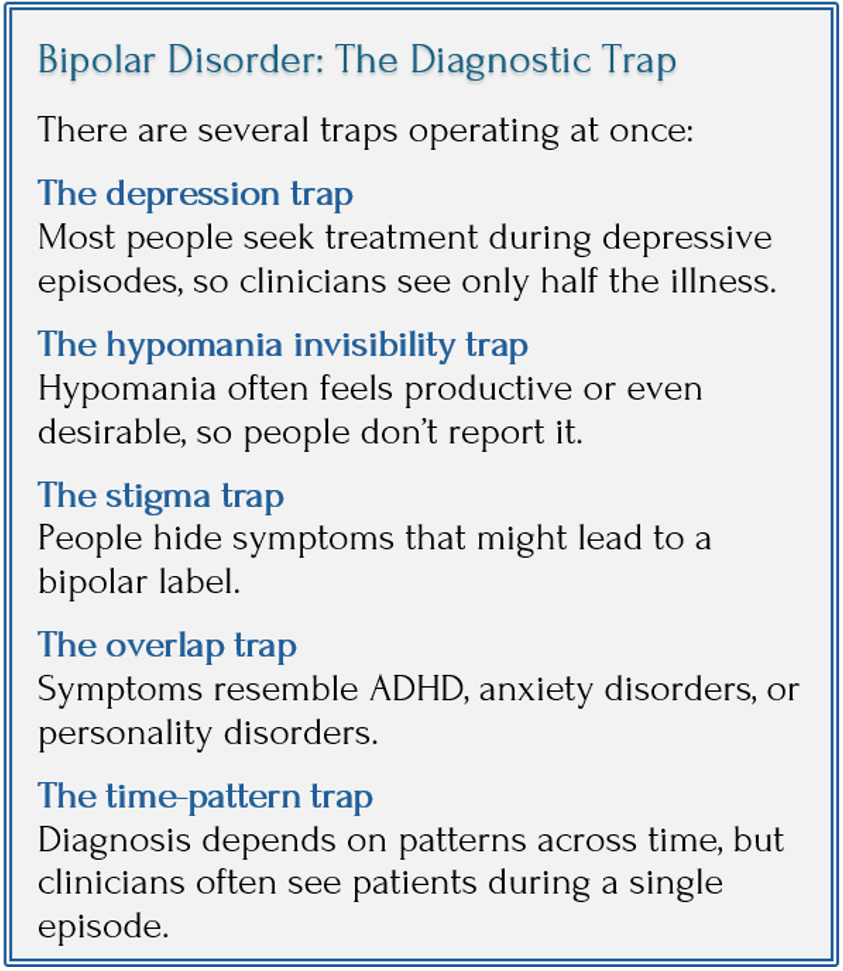
In sum: Bipolar disorder can be difficult to diagnose for several reasons:
- It hides in plain sight: depression tends to dominate the course of the disorder, while hypomania may go unrecognized or unreported.
- Stigma discourages people from speaking openly about symptoms that might suggest mania.
- Early biological vulnerabilities may remain invisible until stress or life changes push the system out of balance.
But another factor also plays a role. Bipolar requires careful assessment over time, and many clinicians don’t receive extensive training in identifying its subtler forms. When symptoms are evaluated quickly or in isolation, the broader pattern can be missed. For this reason, many mental-health specialists recommend a formal diagnostic evaluation — often by a psychiatrist or a doctoral-level psychologist — when bipolar disorder is suspected.
Even when bipolar disorder is suspected, another challenge remains. Comorbidity, the subject of the next post.
On Caregivers: You and Me

In the realm of healthcare, there are many unsung soldiers — the spouses, parents, and adult children of individuals needing care but who may also bear the brunt of abusive treatment. The NAMI survey contributed to our understanding that all of us who are caregivers might go unsung, but we are also deeply affected by the toll it takes on us. I won’t spend further time on this topic, except to say we must invest in ourselves more than we probably do.
Coming Up Next

Many people with bipolar symptoms also show traits that resemble other conditions, particularly attention-deficit/hyperactivity disorder (ADHD) and certain personality disorders, like borderline personality disorder (BPD). [See post 12 for discussion about BD and narcissism personality disorder.] These overlaps can blur diagnostic boundaries and make an already complex illness even harder to recognize. In Post 14: When Diagnoses Overlap: Bipolar, ADHD, Borderline, I’ll look more closely at how these conditions intersect — and why distinguishing them can be one of the most challenging aspects of bipolar diagnosis.