On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
7. When Stress Accumulates

Even as we learn that bipolar vulnerability springs from a well — fed by multiple streams, many genetic — it probably makes little difference to the person buckling from the strain. It’s like a game of kickball, where everyone aims for you (I really hated that game as a kid). Ta this, you can’t get/keep a job. Take that, your relationship is going south. Here’s another blow, you don’t have a financial cushion to pay rent next year. Or, maybe it’s your child being in trouble or your parent cutting you off. You haven’t eaten or slept. The last kickball that brings you to your knees is mental confusion — being so overwhelmed you’ve no idea what to do and no one to ask for help.
Stress accumulating for someone with bipolar disorder is like being pummelled by kickballs. Each ball doesn’t hurt too much on its own, but all together they become too much for the person standing there. Sometimes nothing dramatic happens, just too many things for too long. Conflict, loss, maybe a stray comment or look, illness, success that comes with pressure — in a sensitive system accumulation is what tips the scale.
My Son Today
When I’ve written about my son Jaden’s ordeal with bipolar disorder, I’ve focused on the first diagnoses and hospitalizations, some 12-13 years ago. I haven’t updated the story so far because, unlike other published tales people like to tell, it doesn’t resolve. His variety of BD-I is grindingly severe. It sticks to him like his shadow, never giving him a break. He has a number of comorbidities, including ADHD and PTSD, but I suspect others as well, which compound symptom severity and resistance to therapies,
Jaden is not all that forthcoming to me. He’s not open to psychotherapy, though he speaks with a spiritual counselor when he’s very stressed — which is often. I believe he has made progress, moving over the years from active suicidal ideation to building a life with his partner Ria and a house full of pets that they love like children. While he speaks less of suicide, it’s not far from his thoughts.
Part of the story is his continued financial dependency on me. This was manageable when I was working, but now that I’m retired it’s put me back on my heels. It’s certainly the main reason for friction we experience. To Jaden’s credit, he has been preparing to reenter the job market, but I have no idea if he’ll succeed. He’s more than capable, but because of the stress of meeting the demands of a 40-hour work week.
In this post, as I talk about the impact of accumulating stress, I can speak firsthand about the weight of meeting society’s demands to be self-sustaining. If I were to produce a visual here, my son would be the center figure surrounded by stress bubbles: financial, relational (with me), ADHD attention issues/confusion, nonroutine days (erratic sleeping/eating), no exercise, and no clinically appropriate care. He has a stress load that would be hard for anyone to handle, but for him threatens him daily with acute mania that would send him back to the hospital.
What I see in my son’s daily life mirrors what researchers describe when they talk about accumulated stress lowering threshold. I long to see my son settled into a life that works for him. I’ve asked him to contribute to the blog and hope he will at some point – there will always be space.
If You’re Overwhelmed Right Now, Here’s Why
In the last post, we looked at ignition — how stress meets vulnerability. Here, we look at what happens when stress doesn’t come once, but repeatedly. Specifically, I’ll raise the nongenetic side of BD stressors and triggers.
The question that naturally follows is about what repeated stress actually does to the bipolar brain and body over time. The most recent research increasingly points to patterns of sensitization — where childhood adversity, chronic or acute stress, and disrupted bio- and life-rhythms leave lasting marks on a person’s ability to regulate their mood.
A researcher (cited below) writes, ”It isn’t stress alone that destabilizes mood, but disruption to the rhythms that organize daily life…. For some people, bipolar episodes emerge not from trauma or temperament alone, but from repeated disruptions to sleep, routine, and social timing.” In other words, it isn’t just what happens to us — it’s what happens to our timing systems when it does
Robert Post, “The Kindling/Sensitization Model and Pathophysiology of Bipolar Disorder,” Cambridge University Press
When Repeated Stress Changes the System
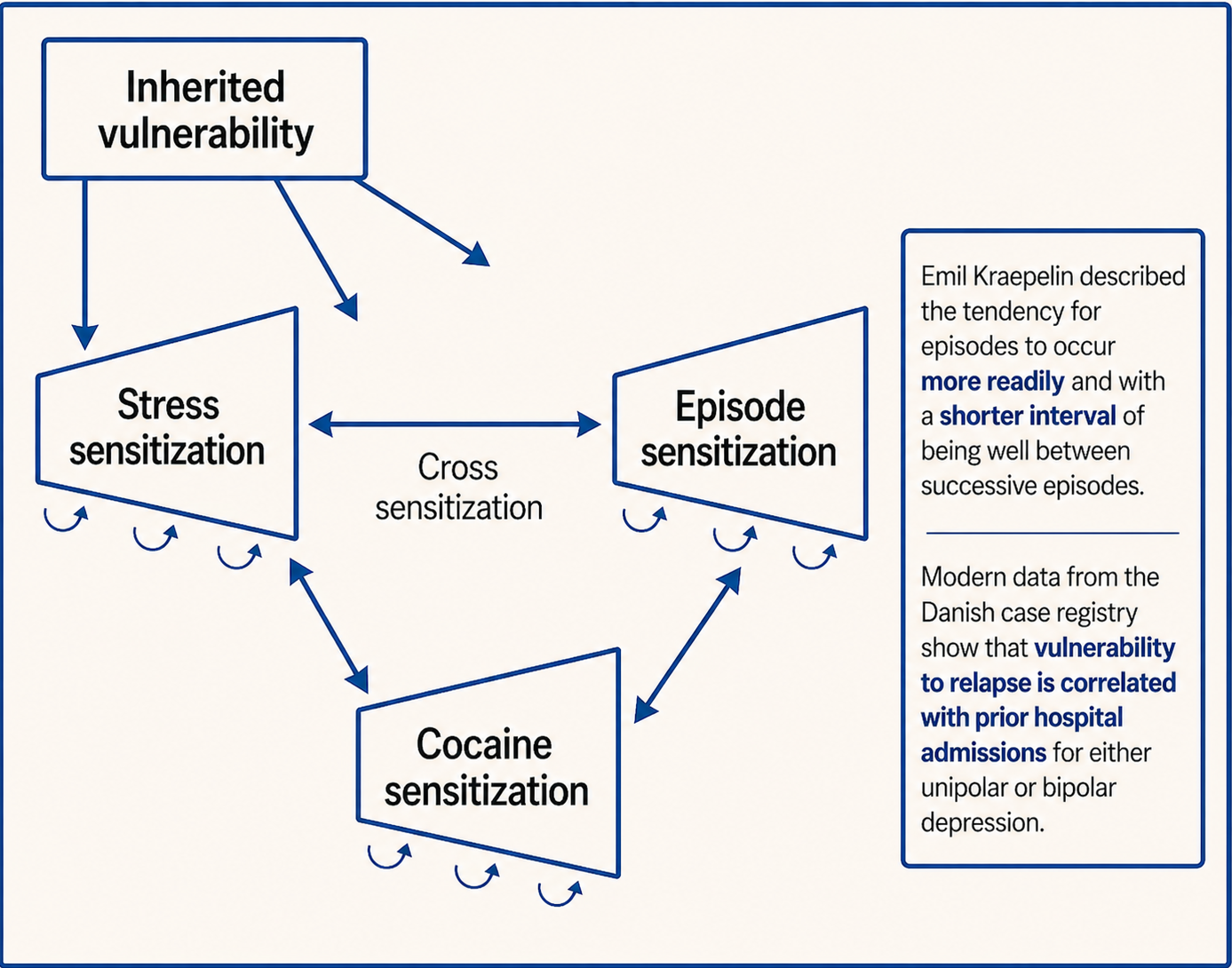
When stress happens once, the system may recover. When it happens repeatedly, the system begins to adapt — and not always in helpful ways. Researchers call this sensitization: the gradual lowering of the amount of disruption a person can absorb before tipping into a manic or depressive episode. Over time, the brain and body don’t just react to stress — they change in response to it.
Life Events Influence How Bipolar Unfolds —Interacting Biological Systems
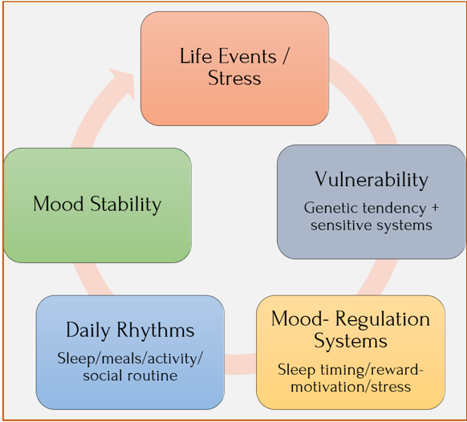
Bipolar disorder involves a combination of vulnerability and environmental stress. Researches increasingly view the illness as a system in which brain regulation, stress, and daily rhythms interact to influence mood stability.
These and numerous other studies show life events affect both bipolar’s onset age and the course it takes. But they affect BD unequally. Mania isn’t always triggered by bad things happening, for example. Sometimes it’s triggered by too much activation, even if positive:
- Positive events (success, achievement, reaching goals) are especially likely to precede mania
- Negative events can precede both depression and mania
- Loss (parent’s death, bad breakup) is surprisingly often linked to mania
- Physical illness more often precedes depression
When Repeated Stress Changes the Course of Illness
As researchers began studying how repeated stress and repeated mood episodes affect bipolar systems, another idea gradually emerged:
bipolar disorder may unfold across different stages over the course of a person’s life.
This framework is known as a clinical staging model. Like staging used in other areas of medicine, it describes patterns that often appear over time. It doesn’t mean everyone follows the same path, nor that progression is inevitable. Many people remain stable for long periods, especially with effective treatment.
In simplified form, researchers often describe three broad phases:
Early vulnerability stage: Genetic predisposition, temperament traits such as high reward sensitivity, and environmental stressors create a system that is more reactive to disruption. At this stage, mood episodes have not yet clearly emerged, but there can be indications of sleep loss, life stress, or circadian instability [see posts 8-9].
Prodromal stage: Some individuals begin showing subtle warning signs before a first manic or hypomanic episode. These early signals — prodromal symptoms — can include:
- Unusually rapid mood shifts or emotional intensity
- Irritability or agitation beyond typical adolescent swings
- Bursts of high energy or reduced need for sleep
- Racing thoughts or pressured thinking
- Periods of unusual goal-driven activity or risk-taking
- Recurring subclinical depression
Each of these can appear in ordinary adolescence. What tends to raise concern is persistence, intensity, or clustering of several signs together, particularly when combined with family history. Looking back, many families can identify early warning signs. But others experience what feels like a sudden storm — the first episode appearing with little warning at all.
Episodic or recurrent stage: Once clear manic, hypomanic, or depressive episodes begin, they may recur over time. Early episodes are often strongly linked to external triggers such as sleep disruption, stress, or major life events.
Over time, researchers believe repeated episodes and repeated stress may gradually lower the system’s threshold for mood instability, meaning episodes can occur with less obvious external triggers. This is also known as a sensitized stage.
Importantly, this pattern is not inevitable. Many people remain stable for long periods, especially with effective treatment and good rhythm regulation. But the staging model helps researchers understand why early recognition and treatment may matter so much.
The Kindling Hypothesis and the Decay Model
Bipolar disorder’s core feature is dysregulated mood states, which cause difficulties with concentration, thought, energy, and behavior. They’re often accompanied by changes in sleep and eating patterns and can last for hours, days, weeks, and even months.
Although BD is distinctive from major depressive disorder (MDD), acute anxiety, or other serious conditions, it’s still frequently misdiagnosed. Here are the main mood classifications defining bipolar spectrum conditions:
One mechanism believed to contribute to this shift in sensitization is something bipolar researchers call the kindling hypothesis. This is when life events and early life stressors together can gradually change how the brain responds to future stress. Like a fire that becomes easier to start each time because the kindling doesn’t cool all the way down, the threshold lowers. In other words, it’s requires less and less to trigger mood episodes.
Supporting the kindling hypothesis is the decay model, which suggests, as people mature, life events often lose some of their destabilizing power — possibly because they strengthen their coping skills and become more resilient. Though experience and time dampen impact, vulnerability still remains.
Here’s a paradox to consider: whether life events cause episodes or whether illness causes life events. Research suggests some life events are consequences of mood episodes. But many events occur independently of the illness.
- Early episodes are more sensitive to external triggers.
- Later episodes become more autonomous and internally driven.
This is What is Meant by "Threshold"
Threshold is meant to convey the amount of disruption a system can absorb before tipping into an manic or depressive episode. Early on, it may take a major event. Over time, repeated stress can lower that threshold, meaning smaller disruptions, like disruptions to sleep or routine, are enough to trigger mood instability.
The gradually lowering threshold is what’s so vexing about bipolar disorder. It’s like the mind–body–brain system remembers.
Repeated Stress / Episodes Lower Threshold
The diagrams below show how the threshold for mood episodes changes over time.
EARLY BIPOLAR DISORDER:
Higher Threshold (More Protection)
LATER BIPOLAR DISORDER:
Lower Threshold (More Sensitization)
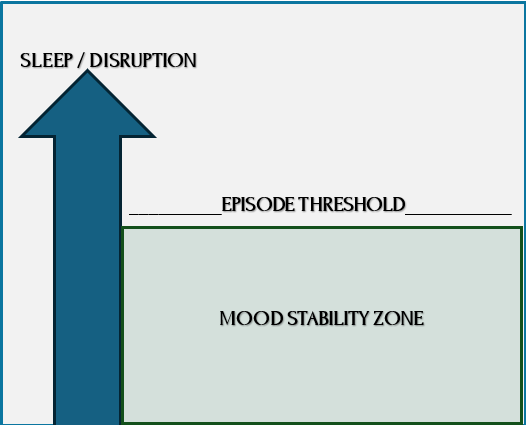
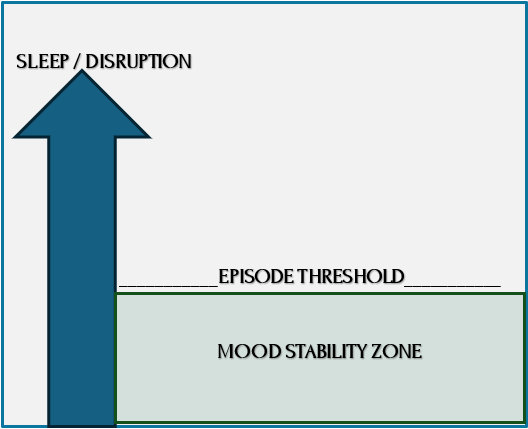
Mood stability zone = System remains regulated. Bipolar research often describes mood stability in terms of an episode threshold — the level of disruption the system can absorb before tipping into mania or depression. Upward arrow = Pushing upward from smaller to larger disruptions.
Crossing the episode threshold line = When regulation fails and episodes begin.
A higher threshold (left) means the system is more resilient — large stressors are required to trigger episodes (severe sleep loss, major crisis).
A lower threshold (right) means the system has become so sensitized by repeated episodes or prolonged stress that it’s easier for smaller disruptions (sleep loss, schedule change, stress) to trigger an episode.
What Specifically Lowers the Threshold
If repeated stress can lower threshold, the next question is obvious: what kinds of stress matter most? Research suggests not all disruptions carry equal weight. Certain experiences — especially those that disturb safety, sleep, rhythm, or stability — appear to act more powerfully on vulnerable systems.
By now, it may not be surprising that environment matters — but it matters in surprisingly specific ways. Given the genetic predisposition that must be there, environmental and lifestyle-triggered situations or circumstances can initiate or exacerbate mood episodes. Researchers now think less in terms of single causes and more in terms of accumulating and diverse life events that act on vulnerable systems.
Childhood trauma
For some people, early trauma becomes part of their story. In fact, trauma stands out as the strongest, nongenetic environmental risk factor for bipolar. The research team writes, “For many people, bipolar disorder unfolds in the context of early adversity — not just biology alone…. Childhood trauma is associated not only with onset, but with a more severe and unstable course across the lifespan.”
This doesn’t mean trauma causes BD. It’s highly individual, with many experiencing trauma who don’t develop BD and many with BD who have no identifiable trauma history. But when trauma and vulnerability intersect, the illness tends to take a more severe course.
Evidence proves early trauma doesn’t just increase risk but seems to reshape the illness itself. Across multiple reviews, childhood trauma is associated with earlier onset age, more frequent episodes, rapid cycling, psychotic features, higher suicide risk, and greater substance misuse.
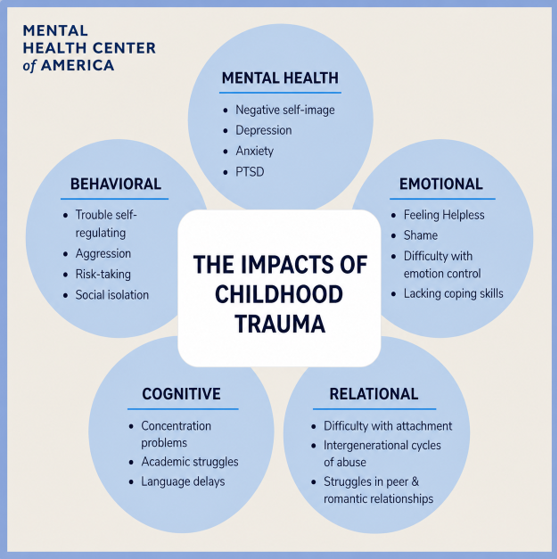
Source: Mental Health Center of America
Among some specific findings:
- PTSD occurs in 16%–39% of people with BD.
- About half report some form of childhood trauma — even without meeting PTSD criteria.
- There’s also a painful feedback loop. People with BD may acquire new trauma during manic episodes, due to risky or disruptive behavior.
- I’d add a personal observation here: there can be additional trauma in how a person in a manic state is treated by poorly trained officials when being taken for care.
Biological Effects of Trauma
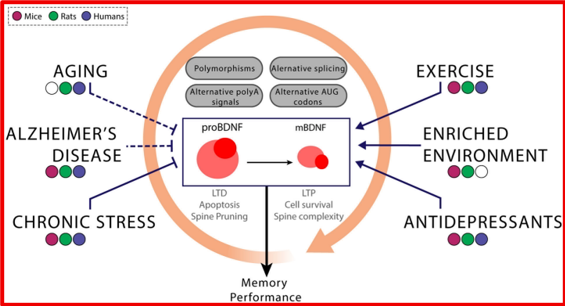
Trauma, Bipolar Disorder, and Reduced BDNF: BDNF levels are dynamic, influenced by both genetic vulnerability and environmental conditions. Chronic stress, aging, and neurodegenerative illness may reduce BDNF, while exercise, enriched environments, and some treatments may enhance it. Source: Magdalena Miranda, “Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain,” Frontiers
In adults, trauma-related biological changes show strong evidence of a link to BD symptoms. It affects both “brain systems and stress biology.” Here are some ways the researchers have identified where biological changes are associated with trauma in BD:
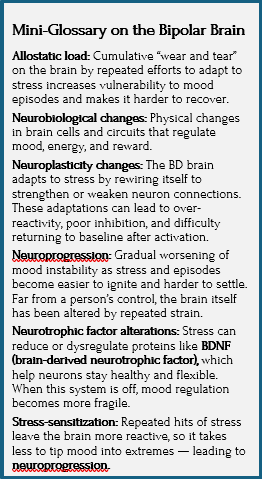
- Reduced BDNF (brain-derived neurotrophic factor): Trauma in BD is associated with lower levels of this critical neuroprotective protein, potentially impairing the brain’s capacity for neuron survival, adaptation, learning, and recovery from chronic stress.
- Altered stress hormone systems: The hypothalamus-pituitary-adrenal axis (HPA axis) is the body’s primary stress-response mechanism. HPA axis dysfunction leads to persistent, toxic levels of cortisol and an inability to return to a calm state.
- Increased inflammation via changes in genes/neurotransmission: Chronic stress can alter gene expression (without changing DNA itself), sometimes silencing protective pathways.
- Shortened telomeres (accelerated biological aging): Chronic stress causes the protective caps on the end of chromosomes (telomeres) to break down faster, signaling the body’s cells are aging prematurely.
Trauma can also worsen unipolar and bipolar depression by damaging relationships. People with trauma histories tend to experience more chronic interpersonal stress and have more severe depressive episodes. So it seems trauma doesn’t just add stress — it reshapes lived experience in ways that feed depression.
For anyone recognizing themselves in any of this — loss, disrupted sleep, overextension, early wounds — it’s important to pause here.
Accumulation, sensitization, or trauma are not failures nor weaknesses — this is what happens when a sensitive nervous system lives in a demanding world.
Climate and Season

It might not surprise those who struggle with depression that seasonal and light-related effects strongly affect mood regulation, likely through circadian rhythms. A large review found a reliable link between seasonal patterns and bipolar symptoms. Not everyone is affected this way — but those who are tend to have a more severe course:
- Mania peaks in spring and summer, with a smaller peak in mid-winter.
- Depression is more common in winter and spring, especially shortened daylight.
- Other climate factors linked to relapse include daylight hours, temperature, and hours of sunshine. This connection is supported indirectly by the fact that light therapy helps mood disorders, suggesting sunlight affects underlying biology.
These seasonal effects likely operate through the same circadian timing systems that I’ve already mentioned and will talk about more in the next two posts.
Social and Work Triggers
Manic episodes often immediately follow heightened disruption, as in interpersonal conflict, financial crises, work stress or failure, or job loss. Being unemployed at the time of illness onset is linked to a higher relapse risk and more psychotic symptoms. Interestingly, a person’s social status (class or background) before illness doesn’t seem to affect BD’s long-term course.

Source: “Jobs Lost to AI Won’t Return,” Forbes
Number of Life Events Predicts Depression
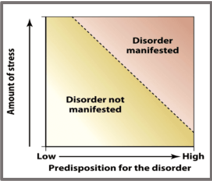
Source: Andrew English, PhD, “Diathesis-Stress Model,” Practical Psychology
We tend to assume big events matter more than small ones. Minor stressors usually don’t shift mood much, but severe life events — or many events in a row — do. However, what counts as major vs minor is subjective. People’s perceptions of their experiences matter.
The number of life events predicts depression. In the strongest study cited (222 patients with BD), more than 60% had at least one major life event in the six months prior to a new episode. The risk of depression increased with the number of events — but whether events were good vs bad didn’t matter. Quantity did.
Also strongly noted is cannabis and stimulant use, especially in genetically vulnerable individuals, which can precede onset, lower onset age, and increase conversion from depression to BD. Cannabis use in particular is enough of a question in people’s minds to merit more attention [see post 11].
Mixed or No Evidence for Bipolar Disorder
Some proposed risk factors (birth complications, infections, maternal smoking, urban living) show inconsistent evidence. They may contribute in some cases, but they do not appear to be central drivers in most people’s bipolar course.
Taken together, these findings suggest that bipolar disorder is shaped not just by inherited vulnerability, but by how stress interacts with the body over time.
What This Means for the Brain — and for You
Repeated stress doesn’t simply trigger episodes — it can gradually reshape the systems that regulate mood, energy, and timing. Understanding this shifts the conversation. Understanding this shifts the conversation. The goal becomes protection: strengthening what stabilizes the system and recognizing patterns early.
Neurobiological Changes
Ongoing stress can physically change how brain cells communicate and regulate mood, energy, and reward, going beyond the psychological stress that might cause anxiety in another person. The point here is that repeated or intense stress is more than a trigger — it actually reshapes brain functioning over time.
The rewired brain can stabilize into patterns that are hard to reverse, altering an individual’s ability to steady their mood swings — as if their brains are too easily revved up and not good at braking.
More than Inherited Genes + Random Life Stress
This research opens wide any preconceived idea we might have had about the nature and nurture of bipolar disorder. More than genes plus random life stress, bipolar disorder emerges as a system-wide condition, taking into account:
- Biological rhythms (the body’s internal timing systems for sleep, energy, and alertness)
- Social structure (regular routines, roles, and stabilizing relationships) in support of those rhythms
- Baseline activation level (how strongly a person’s nervous system responds to stimulation, goals, and reward)
- Effects of cumulative life disruption (gradually accumulating strain caused by repeated changes, losses, or instability)
In future posts, I will talk about how a person may carry a latent vulnerability or predisposition before any symptoms appear, which only becomes illness when life repeatedly disrupts circadian rhythms, ambitious goals (reward-driven pursuits that increase activation), sleep, and social synchrony (alignment between the person’s daily rhythms and those of others).
Events Happen and No One’s to Blame
If we’re not paying attention, these risk factors can easily slide into self-blame or regret. After all, It can feel like a colossal pile-on for one individual, who was born healthy and didn’t deserve this lifetime affliction. So it’s important to say this time to time. The goal is to recognize patterns early and protect what is stabilizing. To understand why bipolar disorder so often unfolds the way it does, why people miss early signs, and why diagnosis can feel like both a shock and a relief. Identifying risk is not about fault finding. Hopefully, it can lead a person who feels beaten down by this illness to restore their agency, have self-compassion, and see next steps more clearly going forward.
Coming Up Next

Researchers write, “When the structures that hold a day together fall apart, mood often follows.” If stress, sleep disruption, trauma, substances, even success itself weaken the terrain, what strengthens it. A person with bipolar needs protection from the environmental factors most responsible for stressing the system and making it vulnerable. Post 8: Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
Sources