On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
4. How Bipolar Risk Takes Shape

Diego Velázquez, Las Meninas (Family of Philip IV), 1656, Museo del Prado, Madrid [detail, see below for full version]
There’s no single cause, gene, or moment for bipolar disorder (BD) to appear. There’s also no particular life event that can “cause” bipolar disorder by itself. But mental health researchers have identified a number of contributing causes — or risk factor — and their various interactions that go a long way to explaining bipolar disorder.
When professionals use the word “risk,” they’re not talking about danger or making bad decisions. Although “risk-taking” can be a symptom of manic behavior, that’s not how it’s meant in this context. Here, that is, in neuropsychological research, risk means the increased probability — not certainty — of the illness and mood episodes showing up.
Risk is Not Destiny
“Risk is not destiny,” experts say, but it’s not evenly distributed either. Understanding bipolar spectrum conditions begins perhaps by understanding mood swings and how severe they are, how disabling they are. But understanding the disorder itself means stepping away from obvious explanations and taking in the entirety of what’s actually happening.
Risk factors affect how severe the illness is (a person’s biological sensitivity) and how frequently the episodes recur (their lived experience). Some people inherit a nervous system that reacts more strongly to disruption or incidence. Others encounter environments that repeatedly push their “systems” beyond what they can regulate.
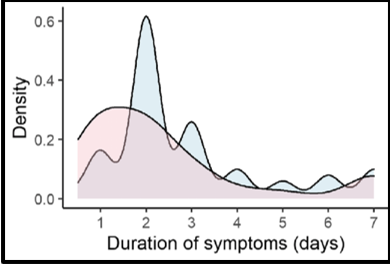
Probability curve for illness. Research Gate
Research is catching up to this “systems’ view of bipolar disorder, looking into the genetics, biology, and life aspects that help explain why this disorder is so disabling. This is welcome news, but patient care hasn’t caught up—and most people with bipolar are not getting the care they need, don’t know what that care should even look like, and may sadly give up without trying.
Specifically, risk factors affect the neurological and physical responses to BD triggers, including single stressful events, cumulative stress, or no discernable event at all. Science is learning more about how genetic complications, neurochemical imbalances, and long-term environmental risk factors interact. Together they can overload the brain and trigger episodes in sensitized systems Here’s what most researchers agree are contributing risk factors in combination:

Sara Solovitch, “The Family Tree: Is Bipolar Disorder Hereditary?’ BD Hope, provided these sources:
Nationwide study of Finnish same-sex twins found high heritability of BD-I, The American Journal of Psychiatry.
If one identical twin has BD, there’s a 70% chance the other twin will develop it — 2-3x the rate for non-identical twins. Stressful or traumatic events can also trigger BD episodes in people who are genetically vulnerable. American Academy of Children & Adolescent Psychiatry (AACAP)
“Bipolar disorder is one of the most clearly heritable disorders there is. The evidence is absolutely overwhelming,” says Samuel Barondes, MD, professor emeritus, Weill Institute for Neurosciences, University of California, San Francisco, JAMA Psychiatry
Genes Set the Stage, But Life Pulls the Curtain
Genetic vulnerability shapes how responsive our brains are to stressors both internal (sleep deprivation, other illnesses) and external (loss, substances). Environmental factors can only contribute to (not cause) BD by how they affect this underlying sensitivity. This explains why two people can live through similar events and emerge very differently. It’s also why two people with the disorder can also react differently.
In some families, bipolar disorder runs through the generations as invariably as freckles or cleft chins appear in other family trees. Even so, looking for your family’s source of bipolar disorder can be a little like searching for the headwaters of the Nile. You start backtracking through the generations and suddenly realize that the “quirky” behavior you once brushed aside as your grandmother’s eccentricity was really a signpost. —Sara Solovitch, “The Family Tree: Is Bipolar Disorder Hereditary?’ BD Hope
Despite irrefutable proof of how inheritable bipolar is, most of us don’t or can’t connect the dots in our family history. But here’s a story where they did just that.
Meet Emma and Patrick: A Family with Passed-Down Bipolar Disorder
This is one of Solovitch’s most compelling profiles [lightly edited for brevity]:

I am exhausted. It’s clear on my face. All moms are exhausted, I know and respect this. But when you add the bipolar layer into the mix, you are in a constant battle with your own mind. People underestimate the physical impact this disorder has. It’s exhausting…” — Shelley A., photograph, The Mighty
When Emma from San Diego scrutinizes her family tree, she traces her BD to her paternal grandfather, a charismatic fellow who could never hold down a job…. It was left to his wife, Emma’s grandmother, to beg the boss to take him back.
But Emma considered her father, Larry, to be the real link. Just like his own father, Larry had trouble holding onto a job. He did, however, keep his kids in check through a combination of fear and play. “The way he played with us was very manic, tickling and chasing us, or locking us out of the house till someone got hurt,” Emma recalls.
Whenever he was home, Emma was on high alert. Her father could lose his temper without warning, screaming, throwing objects, and tossing his kids across the room. Like the time her brother, age 8, received a letter from a foreign country and ripped the stamp while opening it. Her father was enraged and showed it. Why? “Because he was a stamp collector,” Emma says. “And a coin collector. And a camera collector. And a gun collector.”
Many years later, when Emma’s son, Patrick, was diagnosed with BD at age 13, her father — who had consistently refused to see a psychologist or psychiatrist — read over the list of symptoms and nodded, saying, “Yeah, that’s me.”
For a while, an antidepressant seemed to help Patrick. But then he couldn’t sleep, prompting the psychiatrist to prescribe a sedative. “And that sent him over the edge,” says Emma. “So here I had a child who was unable to function. He’d just lie on the floor of his room, asking, ‘What’s the matter with me, Mom?’”
After the difficult high school years — during which he was diagnosed — Patrick quit school at 18, discovered cocaine, and began stealing. “He just went completely over the edge with cocaine, meth, and alcohol,” says Emma. “We finally got him into a treatment program after he had two drug possession charges.”
Although Patrick was the first in the family diagnosed with BD, Emma was the first to be diagnosed with a mental illness. Decades ago, she’d learned she had anxiety disorder. Eventually, her younger sister was also diagnosed with bipolar. “My sister really struggles,” Emma says. “She has four grown children and two of them have been diagnosed with bipolar, too, and are on and off their meds.” —Sara Solovitch, “The Family Tree: Is Bipolar Disorder Hereditary?’ BD Hope
Solovitch writes that Emma no longer feels guilty or responsible for passing along the “bipolar gene” to her son. Emma and her husband go on to become peer counselors, after taking a family-to-family course offered by National Alliance on Mental Illness (NAMI).
More than Symptoms, Mood Episodes Change the System
Research and lived experience make clear that bipolar mood episodes are not only expressions of the illness, but they contribute to its course.
This is meaningful for a person trying hard to get their life on track, because untreated bipolar’s risk profile isn’t promising. After repeated and accumulating disruptions to sleep, routine, and stress regulation, the BD brain can become more easily activated — meaning a lowered threshold for further destabilization. Episodes may require less provocation than before. There may be less time between episodes and, over time, they might not even require external stressors to be triggered.
This is what scientists call kindling, borrowing a term from neurology. And just like lighting a fire, over time the bipolar brain needs less and less friction with a sensitive system to ignite an episode. In time, the system is primed to need no kindling to light the first. Episodes occur more autonomously, driven by internal neurobiological changes.
Another way to look at this is to think of a bridge that can hold steady under ordinary traffic conditions. But after years of semi’s crossing the bridge, high winds, and missed repairs, the cumulative strain begins to weaken the structure. And even with some stabilization, the weakened bridge may not return to its original self.
In sum: Bipolar nervous systems are more reactive. They amplify stimulation, reward (motivation and salience), and disruption more strongly than the non-bipolar system. This doesn’t mean BD inevitably worsens. But it does mean repeated destabilization can leave a nervous system more reactive than it once was, paving the way for future episodes, making it harder to heal.
This is the most compelling reason science has to offer for why early recognition, stability, and effective care matter — and why prevention requires a biological solution, not just a psychological one. If stress and sleep disruption lower the brain’s stability threshold over time, then protecting stability is not optional. It becomes central
Predicting Bipolar — Soon to Come
Although the genetic component of bipolar is undeniable, the relationship isn’t straightforward, physician Barondes (quoted by Solovitch) says. There are an untold number of genes responsible, many of them overlapping with schizophrenia.
As of yet, it’s not possible to predict whether or not someone will inherit or manifest the disorder, but a 2022 study (Nature Genetics) indicates it might happen. Researchers identified a gene (AKAP11) that’s a strong risk factor for both BD and schizophrenia. They also confirmed BD risk is polygenic (influenced by more than one gene) and heterogeneous (diverse in character). In their study of nearly 42,000 BD cases, researchers identified 64-associated genomic loci — specific locations within a genome (contains all an organism’s genetic information) — finding 15 genes significantly linked to BD.
In 1910, Jean-Marc Côté and a team of illustrators created a set of illustrations — named En L’An 2000” (in the year 2000) — some more accurate than others. “Electric scrubbing” coincided with the development of robotics technology. In 2026, my Roomba is vacuuming my house. Prediction is hit or miss, but the hits prolong healthy life. Source: The Vintage News
Genetics overlap with other psychiatric disorders — especially schizophrenia, depression, and autism, as well as anxiety, drug abuse, ADHD, and personality disorders — making it difficult to isolate what specifically puts a person at risk for bipolar. Researchers aren’t sure if it’s high levels of diversity among those with BD or high diversity of the disorder itself, writes Solovitch.
Most individuals who have bipolar disorder can identify someone else in their family who also has a psychiatric disorder. As a point of fact, the other psychiatric disorder is not always bipolar disorder…. Major depression, anxiety disorders, substance abuse disorders, and ADHD are more commonly encountered than is bipolar. People need to think not only about bipolar but other conditions, as well.” —Roger McIntyre, MD, psychiatry/pharmacology professor, University of Toronto; head, Mood Disorders Psychopharmacology Unit, University Health Network, Toronto; quoted by Sara Solovitch, “The Family Tree: Is Bipolar Disorder Hereditary?’ BD Hope
Temperament Signals Early Vulnerability
Most of us know temperament to be about personality. But bipolar research’s version of temperament is about vulnerability. It suggests temperaments are essentially “soft” or milder versions of BD itself. Certain patterns stand out for overwhelming mood regulation: disrupted biorhythms (timing, sleep-wake cycles), intense goal pursuit that puts the system in overdrive, substance use, acute or chronic stress, and early adversity/trauma. These influences aren’t random, but they reveal how tightly mood stability is linked to temperament, energy, sleep, safety, and predictability in a vulnerable nervous system.
A researcher notes, “Temperament reflects early biological sensitivity; whether it becomes a liability depends largely on how well the environment responds.” All people are born with temperaments — basic, stable emotional and behavioral tendencies — that show up very early in life. Temperament is not the same as personality, which develops over time and is shaped by experience.
A child with a “difficult” or highly reactive temperament is more affected by how caregivers respond. If they respond poorly — through rejection, misunderstanding, rigidity, neglect, or overcontrol — the child may adapt in ways that later look like personality disorder traits. This mismatch — between a child’s temperament and the demands of their environment—can lead to maladaptive patterns. No child is born “bad,” but they try to survive psychologically in unyielding environments
Temperament also suggests vulnerability may exist before trauma, so that trauma is acting upon an already sensitive bodily system. In future posts, this understanding of temperament will make more sense in discussion of the hypomanic temperament, reward sensitivity, and circadian instability.
In the next chart, researchers identified five affective temperaments linked to bipolar spectrum conditions:
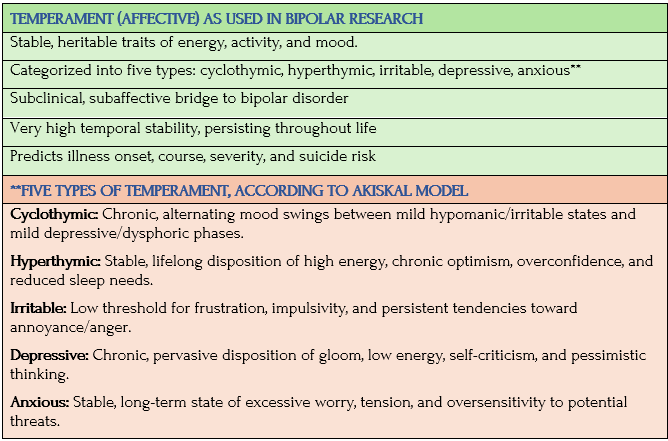
Source: Hagop Akiskal, et al., “TEMPS-A: Validation of a short version of a self-rated instrument designed to measure variations in temperament,” PubMed
This post tried to explain why the human system becomes sensitive long before signs of illness appear — to make it clear that bipolar disorder doesn’t appear out of nowhere. Bipolar risk is unevenly distributed and layered — genes, temperament, and biology shape sensitivity over time. It’s not random, even as it appears like it is. Recognizing these risks is a first step toward seeing how a sensitive mind–brain–body system needs to adapt. In Post 6: A Sensitive System Under Stress, I’ll continue to probe new research to see the frisson between biological vulnerability and sustained stress — often early in life and mostly beyond anyone’s control. This will help us understand exactly how stress acting on bipolar vulnerability can lead to bipolar disorder.
Coming Up Next

This post tried to explain why the human system becomes sensitive long before signs of illness appear — to make it clear that bipolar disorder doesn’t appear out of nowhere. Bipolar risk is unevenly distributed and layered — genes, temperament, and biology shape sensitivity over time. It’s not random, even as it appears like it is. Recognizing these risks is a first step toward seeing how a sensitive mind–brain–body system needs to adapt. In Post 6: A Sensitive System Under Stress, I’ll continue to probe new research to see the frisson between biological vulnerability and sustained stress — often early in life and mostly beyond anyone’s control. This will help us understand exactly how stress acting on bipolar vulnerability can lead to bipolar disorder.
