On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
7. When Stress Accumulates
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
11: Bipolar and Cannabis: Relief, Risk, and Regulation

Photo: Abigail Nover, “Cannabis Use in Bipolar Disorder Presents a Treatment Challenge,” 2018, Psychiatry Advisor
Cannabis sits at a difficult intersection in bipolar disorder (BD). For a person living with the symptoms and stress of the illness, it can feel like relief in the moment. But cannabis also interacts with the very biological systems — sleep, stress regulation, and reward processing — that are already vulnerable in BD. That overlap raises important questions for researchers, clinicians, and people living with the disorder.
For someone with BD, these systems don’t always regulate themselves smoothly. Sleep can fall out of sync. Stress systems can stay activated long after they should settle. Reward circuits can amplify emotional intensity. Using cannabis — a gummy to sleep, a strain to calm racing thoughts — can feel like a way to restore balance. In many cases, it’s an attempt to regulate a system that feels chronically out of alignment.
Relief and Risk Can Both Be True
When Amanda, diagnosed with BD at age 12, first tried cannabis at 16, she felt something she hadn’t experienced in years: quiet.
“No longer do I have these constant mood changes, and my mind doesn’t run a mile a minute with dread and fear.”
Nicholas tells a similar story. Struggling with manic and depressive episodes, he has lost educational and professional opportunities, relationships, and even faced bankruptcy. Before he understood bipolar disorder or had seen a psychiatrist, he began using cannabis in high school.

Photo: Stocksy
“I had never seen a psychiatrist and knew little about mental health, but I did notice that smoking indica-heavy cannabis helped me sleep better and was one of the only methods I had discovered that slowed my manic thoughts to a manageable level.”
Nicholas also uses cannabis to stimulate appetite when depression and anxiety make eating difficult, and as a social activity that helps him stay connected to friends.
Amanda and Nicholas — interviewed at the Southwest Patient Group, a San Diego marijuana dispensary — represent a broader pattern. According to reporting by Abigail Nover in “Cannabis Use in Bipolar Disorder Presents a Treatment Challenge,” Psychiatry Advisor, 2018, cannabis is the most commonly abused substance among people with bipolar disorder. Lifetime cannabis use among bipolar patients is estimated at around 70%, and about 30% meet criteria for cannabis abuse or dependence.
Research also links cannabis use with earlier onset of bipolar symptoms, more frequent mood episodes, increased risk of rapid cycling, poorer outcomes, and lower treatment adherence.

Photo: Stocksy
Amanda and Nicholas find relief in a substance that science suggests may worsen long-term outcomes. Understanding why cannabis can feel helpful in the moment — yet potentially destabilizing over time — is part of the puzzle.
Age may also matter. The adolescent brain is still undergoing major development in reward circuitry and emotional regulation. Some research suggests earlier cannabis exposure may increase vulnerability to mood disorders or shift the age at which bipolar symptoms first emerge.
A Family Experience

Photo: Shutterstock
I also have a story — or rather, my son’s story.
About ten years ago, not too long after Jaden, now 37, was diagnosed with BD-I, I rented a beach house for a family vacation and, frankly, some family healing. Jaden’s partner didn’t join us, but she sent him along with several containers of the cutest pot-laced gummies and mini-cakes I’ve ever seen. They were meant to sustain him since I had said there would be no smoking in the rental house.
The third night in, Jaden offered us a sampling from this impressive display. I asked him how much I should take, given how little experience with these modern, potent edibles. He assumed I asked could take, because he said two pieces — assuming I wouldn’t eat them both at once. My other son, Etan, and his girlfriend each took two.

So I took two.
As I cleaned up from dinner, I felt the buzz coming on and had a brief moment of genuine happiness. My sons were already playing a video game hooked up to the TV, laughing and having fun.
Within 15 minutes, I knew I was in trouble. I could barely longer stand, and everything looked strangely distorted. I quietly made my way to my bedroom, lay down on my bed and didn’t move for the two hours. I didn’t sleep — I just lay there convincing myself I wasn’t dying and that morning would eventually come. When I finally had to use the bathroom, I practically crawled across the floor to get there and back.
During those half-comatose hours, I could hear the three of them having a great time. And then a thought came to me with sudden horror: Is Jaden doing this to himself every day?
The next morning everyone was half concerned and half amused about what had happened to me. None of them had been affected the way I was. In that moment, I was the vulnerable one — someone with no tolerance for the potency of the dose I’d taken.
Over the years, I’ve continue to ask Jaden about his cannabis use and get the same answer. He says he’s hardly affected anymore because he has built a tolerance. Without it, he says, he can’t get through the day. He can’t eat. He can’t function. Alongside his medications, it helps him regulate his daily life.
He now has a medical prescription, and his psychiatrist is aware he uses cannabis daily. But others have raised concerns.
Why Cannabis Can Feel Like Relief
For people like Amanda and Nicholas, cannabis is not primarily about getting high. It’s about evening out a system that feels misaligned, not functional, unsettled.
The brain contains a widespread regulatory network called the endocannabinoid system. It helps modulate many functions relevant to bipolar disorder — sleep, appetite, stress response, and reward processing. THC, the psychoactive component of cannabis, interacts directly with this system.
Because the endocannabinoid system influences so many regulatory processes, cannabis can sometimes create a temporary sense of balance.

Photo: Shutterstock
In people with mood vulnerability, however, cannabis can also amplify the emotional tone already present rather than changing it. A mildly elevated mood may become more energized or expansive, while underlying anxiety may become more intense. Whether this shift is soothing, intensifying, or destabilizing depends on the person, the mood state they’re in, and the surrounding context.
When THC activates the brain’s endocannabinoid receptors, dopamine activity increases in reward pathways associated with motivation and emotional intensity. Certain excitatory signals also quiet down. For someone whose thoughts feel accelerated or overwhelming, this shift can feel like relief.
Cannabis does not cause bipolar disorder. But researchers believe the relationship likely runs in both directions: people experiencing mood instability may turn to cannabis for relief, while cannabis may amplify the biological vulnerabilities that define the illness.
The bipolar brain is already sensitive to changes in sleep, dopamine signaling, and stress response. Cannabis acts directly on all three. That is where relief and risk begin to overlap.
Not All Cannabis Products Are the Same
Another complicating factor is potency. THC is not only responsible for the intoxicating high, but also for the dopamine surge associated with both euphoria and psychosis risk. Today’s cannabis often contains THC concentrations several times higher than found in cannabis from the 1970s or 1980s.
Higher potency means stronger effects on the very brain systems — dopamine signaling, sleep regulation, and emotional intensity — that are already sensitive in bipolar disorder.
Some people seek out strains with lower THC or higher CBD, another component of cannabis that doesn’t produce a high and may interact differently with brain signaling systems. Much of the research linking cannabis to bipolar risk involves high-THC products, while CBD remains an area of emerging study.
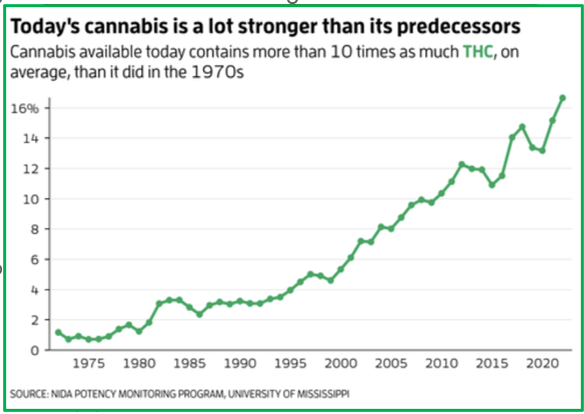
Levels of THC have been steadily rising in cannabis since the 1970s, largely due to growers selecting for more potent strains. Alexis Wnuk, “Is cannabis today really much more potent than 50 years ago?” New Scientist
When Relief Today Becomes Risk Tomorrow
The more complicated question is what happens over time.
One pathway strongly implicated in mania and psychosis is the mesolimbic dopamine system — the brain’s reward circuit. THC increases dopamine release in this pathway. In a sensitized brain, repeated stimulation may gradually lower the threshold for mood episodes.
Repeated activation of these pathways can make them increasingly reactive — a process related to what researchers call kindling, in which mood systems become easier to trigger over time.
Not immediately, nor predictably — but cumulatively.
Research consistently finds cannabis use among people with BD is associated with a more difficult illness course, particularly with high-THC products. Here’s what current research stands behind:
- Increased manic or psychotic symptoms in vulnerable individuals.
- Earlier onset age of bipolar symptoms and more frequent episodes.
- Higher rates of rapid cycling and psychotic features
- Poorer overall prognosis and greater disability.
- Higher rates of cannabis use disorder (CUD).
- Lower adherence to prescribed medications.
- Increased suicide risk in some studies.
Clinicians sometimes see this in their patients as well. San Francisco-based psychiatrist Girish Subramanyan, notes the psychotogenic nature of cannabis:
Cannabis use can complicate BD management by causing mood instability and psychosis in certain BD patients. Cannabis is a known psychotogenic drug for some people, though most people who use it do not develop psychosis…. The possibility of cannabis contributing to manic relapse in BD-I makes it potentially more dangerous in BD-I. —Girish Subramanyan, interviewed by Abigail Nover, Psychiatry Advisor
Sleep Architecture
By now we know sleep plays a central role in mood regulation. From REM to deep dream sleep, structured stages of sleep move across the night in repeating cycles — a pattern known as sleep architecture — which help regulate mood, memory, and emotional stability.
Cannabis can make falling asleep easier, which is one reason people with bipolar disorder often use it. But research suggests THC may disrupt deeper sleep structure by reducing slow-wave sleep, suppressing REM dreaming, and fragmenting sleep cycles.
These changes may not be obvious after a single night. Over time, however, disrupted sleep can destabilize circadian rhythms that help protect against mood episodes.

Photo: Stocksy
Cannabis — Worse than Cigarettes?
Researchers sometimes drawn an analogy to cigarette smoking. Early smokers often reported that cigarettes helped them relax or concentrate. The immediate effects were real. The long-term risks took decades to fully understand.
It seems we’re wired to prioritize immediate relief over distant risk — especially when the relief is tangible and the risk feels abstract.
For someone with bipolar disorder, the relief is felt tonight. The destabilization, if it occurs, may not emerge until months later and can seem to come “out of nowhere.”
When someone you love genuinely feels helped by cannabis, arguing from long-term risk can feel painfully abstract.
Julie Fast’s “Bipolar Significant Seven”
Mental health expert Julie Fast — co-author with John Preston of Take Charge of Bipolar Disorder — was diagnosed in 1995 with BD-II and schizoaffective/psychotic disorder. She developed a management system for bipolar that includes medications, lifestyle, and triggers.
Cannabis appears on her list of substances she calls the “bipolar significant seven.” Her approach is rooted in harm reduction and psychoeducation rather than judgment. Among her observations:
- Substances affecting dopamine can push mood up and then crash it down.
- Many professionals receive little training on substance effects in BD.
- Cannabis messaging is confusing in the era of legalization.
- Today’s THC potency is dramatically higher than in past decades, making addiction possible.
- Because BD can worsen cumulatively over time, even small destabilizing influences may matter.
Cannabis Use Disorder (CUD) Is Not the Same as Heavy Cannabis Use
It’s common to hear concerns about “heavy cannabis use,” which can be confused with cannabis use disorder (CUD). Heavy use refers to how much or often someone uses cannabis, which by itself doesn’t lead to addiction.
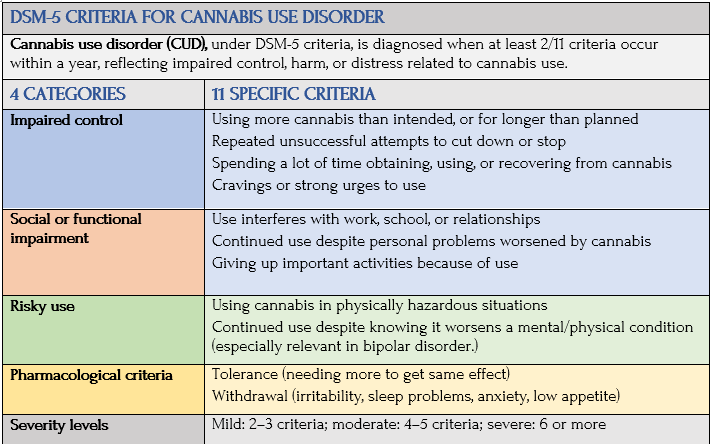
CUD, by contrast, is a clinical diagnosis defined in DSM-5 by significant impairment or distress, including loss of control over use, persistent cravings, continued use despite harm, or withdrawal symptoms.
Some people use cannabis frequently without meeting criteria for CUD. Others develop CUD with lower levels of use.
Even so, research suggests cannabis can destabilize mood regulation before it reaches the level of addiction. The question for many individuals becomes less “Am I addicted?” and more “Is this helping — or making my illness harder to manage?”
Clinically, this is still important in BD, but not the same as diagnosing a disorder. Research consistently shows that cannabis — particularly frequent or high-potency use — is associated with worsened mood instability, increased risk of mania or psychosis, poorer treatment adherence, and more frequent hospitalizations, even in individuals who do not meet full criteria for the disorder.
Here’s the official definition of CUD:
A Clinical Gray Zone
Because cannabis use is so common, many clinicians focus on harm-reduction rather than simple prohibition. Honest discussion, mood charting, and self-monitoring can help people notice patterns of sleep disruption and episode activation.
If I could speak directly to regular cannabis users with bipolar disorder — including my son — I would never dismiss the relief they feel. The desire to sleep, calm racing thoughts, or function through the day is deeply understandable. But I would want them to know the science as well.
This is ultimately an empirical question: what patterns emerge over time, and what leads to the most stable life possible?
Living with the Tension
Stress, life transitions, access to care, and individual biology all influence where someone with bipolar disorder lands. Neither casual experimenter, nor escalating spiral. But steady, intentional, “this helps me” middle.
Those of us who have watched a loved one descend into mania or psychosis know how devastating that unraveling can be. So we live with a tension between compassion and caution. I believe what my son tells me. I can see the relief in his body. But I’m also not neutral about risk. I’m a parent who loves, not a clinician arguing from abstraction. My son has become the living embodiment of this ambiguity.
This is the nature of bipolar disorder. It falls to the bottom of the funnel. There’s nothing romantic or enlightening about it. It’s about managing vulnerability, body rhythms — and sometimes even brilliance.
Coming Up Next

In Post 12: Temperament is Not Behavior: The Biology of Bipolar Vulnerability is for me a fairly pivotal post in my own understanding of mental disorders and how they appear and what they represent underneath. For the first time, I encountered the hypomanic personality — not a person who is hypomanic — but a person who is vulnerable to the disorder developing. I also use the example of narcissism to show how features of bipolar and narcissism can appear to be similar, but come from different places. All of this points to the great care and attention required so people get the right diagnosis and treatment for the best outcomes.