On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
6. A Sensitive System Under Stress

Egon Schiele, Seated Woman With Bent Knees, 1917, pencil/gouache, National Gallery of Prague
In the last post, we looked at the architecture of bipolar vulnerability (called diathesis) — genetics, biology, temperament, inherited sensitivity. But vulnerability alone is not illness. Many people carry risk and never develop bipolar disorder. Others live stable lives for years before their first episode appears. In this post, I’d like to explore what changes. What turns a latent proclivity into a full, disruptive, and frightening illness of cyclical mood episodes.
Researchers describe bipolar disorder (BD) as the meeting point between biological vulnerability and life stressors — both internal and external.
Two people may live through the same loss, excitement, or pressured event and one weathers it, while the other tips into a manic or depressive episode. The difference is not about lacking character or will or being too thin-skinned. It’s a question of threshold — the balloon that can take no more air before bursting, when gathering stressors overwhelm an already overstimulated system.
Repeated destabilization raises vulnerability over time. The brain becomes more reactive, recovery slower, and triggers more varied. But what specifically causes ignition?
Meet Retired Major General Gregg Martin, PhD
In 2003, then-Colonel Gregg Martin was leading thousands of soldiers in Iraq when, as he later wrote, “the intense stress and thrill of combat triggered my genetic predisposition for bipolar, sending me into a high-performing mania.” He didn’t know it at the time, but something had ignited. Upon returning home, he “sank into depression,” and over the next decade his mood “surged higher and sank lower,” undiagnosed and untreated.
Years later, after stabilizing on lithium and entering sustained recovery, Martin experienced an episode that revealed how ignition can still threaten even a well-managed illness.
An exchange of messages with a colleague about the chaotic U.S. withdrawal from Afghanistan became increasingly heated. The subject touched what Martin calls a “no-go/guardrail” topic for him — political decisions that, in his experience, had cost soldiers their lives. “Bad politics helped kill and maim our soldiers in the Iraq War,” he wrote. He knew from experience this could intensify his bipolar symptoms.
Then came the trigger.

Major General (ret.) Gregg Martin, U.S. Army, Psychiatric Times. Photo: G. Martin
Without warning, this topic hurled me back to spring 2003 and into Iraq, where bad political decisions torpedoed our mission and fueled the nascent insurgency. I felt like I was there, in Iraq — the sights, the sounds, the smells, and the hellish environment. I was there, on the ground again with the constant threat of improvised explosive devices (IEDs), rockets, ambushes, snipers, and violent mobs….
In reality, I was sprawled on the living room floor, shaking and pounding my fists, with my breath heaving and heart racing, in an acute panic attack. —Retired major general, US Army, Gregg Martin, PhD, “Beware of Relapse!” Psychiatric Times

Illustration: National Ignition by Ochre
By the next day, he felt stable again, but recognized the danger: “I am fortunate this episode did not trigger a full-scale bipolar recurrence.”
Ignition did not come from weakness or ideology. It came from convergence: a biologically vulnerable mood system, unresolved combat trauma, escalating stress, and entry into a known trigger zone. He later acknowledged, “I engaged with a colleague who became toxic and aggressively pushed a toxic subject.” He had previously built “guardrails” around that topic but allowed himself back into it.
The episode showed how quickly stress can overwhelm a sensitized system. The biological cascade — memory, threat response, adrenaline, cortisol — surged. For someone with bipolar disorder and PTSD, that surge carries risk. A sensitized system can tip.
Martin responded by restoring boundaries. He cut off communication with the colleague and “rebuilt the guardrail.” Since then, he has had no recurrence.
“I will always have bipolar disorder; it will not go away,” he concluded. Even years into recovery, his mental health “burst suddenly” under strain. The lesson, he writes, is vigilance: to know one’s triggers, protect sleep and stability, and treat recovery as a “forever war.”
In his story, ignition is not dramatic at first. It’s a spark — stress meeting vulnerability. And in a sensitized brain, a spark can be enough.
A Many-Layered Condition: The Stress–Vulnerability Loop
Weather is a good metaphor to picture the stress–vulnerability loop in how weather affects the landscape. In calm conditions, hiking up a mountain may give way to beautiful vistas at every turn. But in heavy rain, the paths become dangerously muddy and small streams turn into torrents, making the terrain difficult to traverse with limited visibility. The topography hasn’t changed, but the conditions acting on it have.
Most of our nervous systems can withstand disruption, reversals in our reward system, or unexpected change. But for someone with bipolar disorder, disruption can be experienced as menacing or overwhelming. Stress — whether biological, emotional, or environmental — is the weather acting on the landscape. When stress and vulnerability reinforce each other, the results can be devastating.
The point here is the interaction. Stress doesn’t create vulnerability, and vulnerability doesn’t guarantee illness. Friction doesn’t always ignite or, if it does, we compensate with problem-solving and coping.
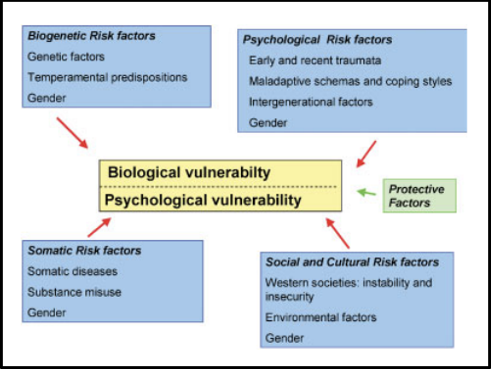
Psychobiological vulnerability for depression: risk and protective factors. Source: Chris Schotte, et al., “Biopsychosocial Model as a Guide for Psychoeducation and Treatment of Depression, Research Gate
None of us are free from experiencing stress. The question is how a sensitive system responds. In bipolar, it’s only when conditions accumulate or intensify does stability become harder for people to maintain.
Stress is Not Just Emotional — It’s Biological
In my blog on anxiety and panic disorders, I described our fight-or-flight response (FFR), the system that has protected us since the beginning of humankind. When we face a threat, multiple brain–body systems fire up. When the threat passes, they calm down.
That’s how it’s supposed to work. The problem in modern life — and in certain mental health conditions — is that stress doesn’t always resolve. Chronic or repeated stress keeps the system switched on. Over time, it doesn’t fully reset. And that has consequences for future health and wellbeing.
Stress as a Whole-Body Chain Reaction
When we experience stress, the body releases hormones — especially adrenaline and cortisol. These chemicals travel through the bloodstream back to the brain and temporarily change how neurons fire and communicate — while influencing mood, attention, energy, and motivation.
How much they change things depends on how intense the stress is, how long it lasts, and which brain systems are already sensitive. At the center of this response is the HPA (hypothalamic–pituitary–adrenal) axis — command central linking the brain to the adrenal glands, which regulate cortisol. Stress also activates the autonomic nervous system and immune pathways.
More than an emotional reaction, it’s a coordinated biological cascade. Chronic or acute stress can also increase dopamine in brain regions involved in motivation and reward, which can have the effect of sharpening our focus and mobilizing our energy. But when the reward system is already highly responsive, dopamine shifts can contribute to unwanted changes in mood, drive, and behavioral activation. This is a reason stress can precede both depressive dips and manic acceleration.
The Bipolar Brain at Rest
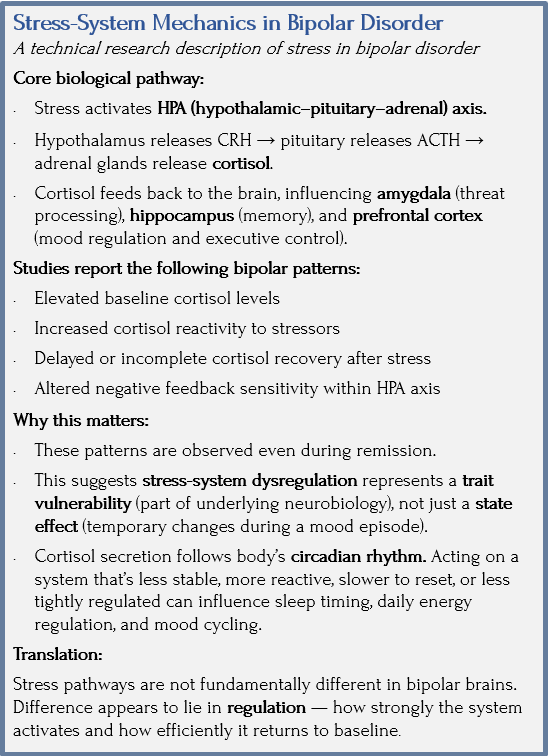
Sources: Eduardo Umeoka, et al., “The Role of Stress in Bipolar Disorder,” PubMed; Stuart Watson, et al., “Enhanced cortisol response to dexamethasone/CRH in bipolar disorder,” The British Journal of Psychiatry (2004), Cambridge University Press
In a typical nervous system, cortisol follows a daily rhythm. It rises in the morning and falls across the day, in close connection to the body’s internal clock. The stress response turns on — and then it turns off. It’s meant to be self-limiting.
When cortisol remains elevated, irregular, or slow to settle, the body’s rhythm shifts. In someone with BD whose circadian system and reward circuits are already sensitive, even small disturbances can alter mood stability.
That’s why sleep is an issue: when it’s off it has an outsized effect on the person with bipolar. Same with energy spiking at the wrong time, which weakens regulation. Reward pathways can become more reactive and disruptive: accelerating ideas, expanding plans, intensifying hope — or it all collapses. This isn’t overreaction in a psychological sense, but a measurable shift in neural regulation.
Research supports this. Studies — including work from the University of Cambridge — show many people with BD have higher baseline cortisol levels and altered stress responses, even outside of mood episodes. In laboratory settings, their stress systems can be harder to quiet and more reactive than expected. This is an especially significant finding, because this pattern shows up even in remission. It suggests stress-system dysregulation may be a trait of the illness — not just a reaction to episodes (state effect).
When researchers compare typical and bipolar stress responses, the basic biological pathway is the same. And like our mountain in the rain, what differs is the regulation — how intensely the system reacts and how smoothly it shuts down.
Meet Writer Michelle Vasiliu

Photo: Psychology Today
In 2007, when I was 40 years old, I experienced my first manic episode and was duly diagnosed with bipolar one.
It is highly likely those sporadic periods of frenzied activity, little sleep, and incredible optimism I’d experienced inbetween debilitating depressive episodes during my teen years were actually hypomanic episodes. My original diagnosis of clinical depression was, in all likeliness, incorrect. The extreme mood swings I had been experiencing for over 25 years were symptomatic of bipolar affective disorder.
So what changed in 2007? What brought on this full-blown manic episode which saw me carted off in an ambulance, screaming and kicking, to the local psychiatric hospital where I was “sectioned” for 6 weeks? Three days of next to no sleep.
I knew something was happening to my body. My eyes wouldn’t focus properly, my racing thoughts became erratic, and I had so much energy it was impossible to slow down, let alone sleep. In fact, sleep was the last thing on my mind. And this is why everything went so terribly wrong.
In my sleep deprived state, my wired, crazed mind was euphoric. I resisted sleep with a vengeance and ignored the frantic pleas of my confused and frightened husband begging me to “go to bed.” As the days went on I became irrational to the point of being delusional. This is when my husband called the crisis assessment team, who sent me to the psychiatric hospital for observation and further assessment.
As obvious as it now seems, in the early days of my bipolar diagnosis, no one, not even the so-called experts treating me, could see how lack of sleep was so integral to my manic state.
It took many years in fact to recognize lack of sleep in combination with excessive activity and the inability to “slow down” as the number one trigger for me in terms of bringing on a manic episode.
Today, having a regular sleep routine is perhaps one of the most important things I can do for myself to stay well. When I find myself struggling to relax or stop those racing thoughts I now put strategies into place to stave off a manic episode. Perhaps the most important strategy is to get a restful sleep come my bedtime. If sleep eludes me, I take a sleeping tablet (I have a small supply in my bedside table for emergencies only).
It is now 15 months since my last hospitalization, after a total of 18 admissions over the course of 28 months. Sessions with my outreach worker made the biggest impact in terms of helping me to get well and stay well. She taught me to look for my triggers and warning signs prior to me becoming unwell.
These days, I do all I can to stay physically and mentally healthy. I try to lead a balanced life by letting go of the stressors in my control. I take my medication religiously. And I pay close attention to my triggers, in particular, a sustained period of little or no sleep and/or a deviation in my regular sleeping routine. I have managed to remain stable for the longest period of my adult life. It is a state of wellness I hope to hang onto for as long as possible. —Writer Michelle Vasiliu, “The Correlation Between Insomnia and a Manic Episode: A Personal Account,” International Bipolar Foundation
Stress, Sleep, and the Amplification Loop
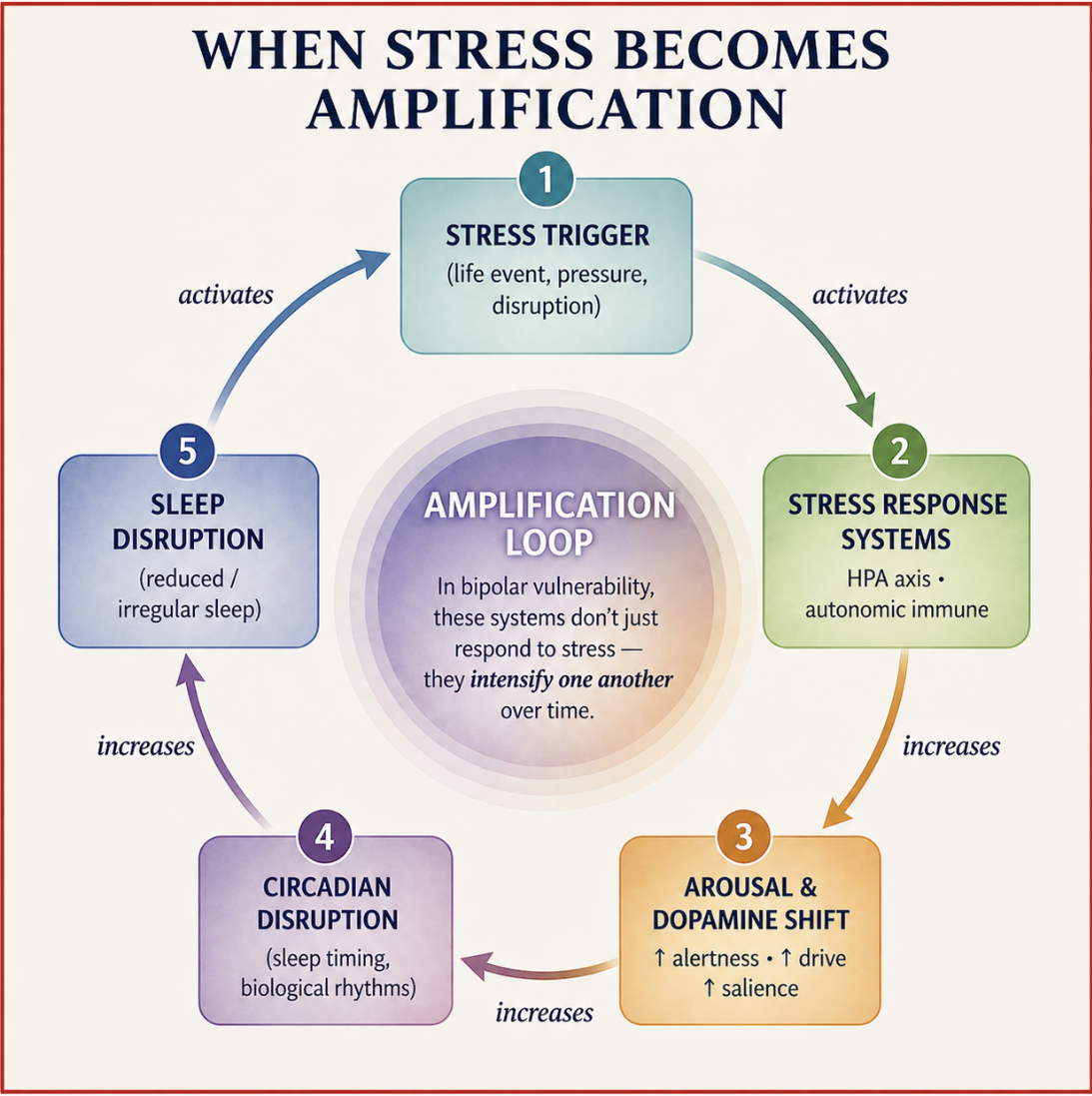
Illustration: Jan Swan and ChatGPT/ai
According to the Eduardo Umeoka team, one of the earliest biological effects of stress is sleep disruption. Elevated cortisol and activation of the sympathetic system delays sleep onset, causes REM sleep to become fragmented, and shifts circadian timing.
Because sleep and circadian rhythms “organize” mood and energy, even modest sleep disruption can have outsized effects in someone whose timing system is already sensitive. They call this the amplification loop.
The researchers also talk about “thresholds,” which means every nervous system can absorb some strain and stay steady. But if stress is intense, chronic, or added to poor sleep or heightened reward activation, stability gives way — threshold is lowered. In bipolar disorder, that point tends to arrive sooner.
There are so many avenues for stress to enter our system. More than emotional and social stress, we’re also physically stressed from sleep loss, illness, pain, success, loss — these ups and downs converge in the brain. In the bipolar brain, this convergence may be destabilizing, not just the impact of a particular incident.
So What Does This All Mean?
Hopefully it’s clear by now that bipolar disorder is not just about mood. It involves at least three interacting biological systems:
In many people with bipolar disorder, each of these systems is more sensitive as an ongoing feature of their neurobiology — a trait vulnerability. With stress, these bio systems do more than react — they amplify one another.
AMPLIFICATION AND REGULATION
Amplification is what happens when interconnected biological circuits are put under strain. I would like every person struggling with self-worth and self-esteem to see this in neon lights. Understanding this shifts bipolar disorder out of the realm of willpower and character and into the realm of biological regulation and vulnerability.
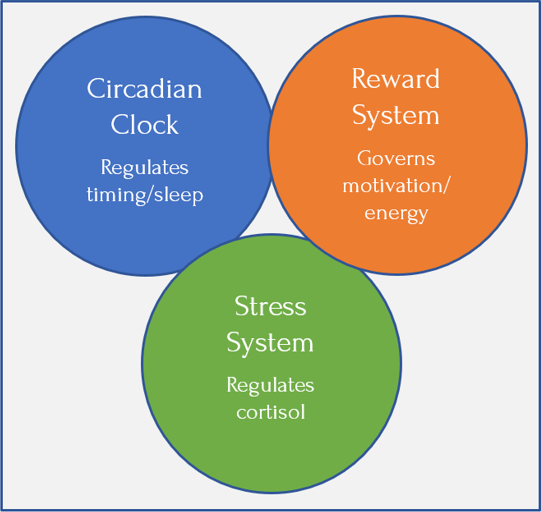
These core systems — circadian timing, reward regulation, and the stress response — don’t operate in isolation but within a broader physiological context that includes immune and inflammatory activity. Any change can influence how these systems function and interact, but this isn’t a fixed condition. Just as these systems can become more reactive under strain, they can also move back toward balance as the underlying state becomes more stable. Graphic: Jan Swan
Bipolar disorder isn’t just different moods, but a complete shift in mindset and energy… You can’t beat yourself up for having bipolar disorder. It’s like being mad at a flower for being beautiful.” — Mental health advocates Marnie Goodfriend and Demi Lovato
I think scars are like battle wounds — beautiful, in a way. They show what you’ve been through and how strong you are for coming out of it. — Demi Lovato

Demi Lovato — recording artist, actress, and mental health advocate — speaks openly about her bipolar diagnosis. She describes her shift in thinking this way: “When I got the diagnosis, there was a sense of relief that came with it, because I thought, ‘I can put a name to this, and this is why.’”
Her relief wasn’t because her difficulties disappeared, but because confusion and self-blame did. Naming it made it possible to understand what had once felt like personal failure. That opened the door to learning how to regulate bipolar.
Novato was executive producer of Beyond Silence, a documentary on three people living with mental disorders. She also launched Be Vocal, a campaign to encourage anyone struggling with mental illness to talk about their experiences. In partnership with The Jed Foundation and the National Alliance on Mental Illness (NAMI)
Regulation is our ability to adapt and maintain and not spin out. It can be supported, even if it’s not under obvious distress. Bipolar is not a collection of symptoms but a systemic mind–body–brain illness. Just as we don’t blame the mountain for the rain, we don’t blame a sensitized nervous system for reacting, often violently, to life’s pressures.

Demi Lovato at Billboard Women in Music, 2024, YouTube Theater, Inglewood CA
Coming Up Next

In Post 7: When Stress Accumulates, I’ll look more closely at the kinds of stressors that most strongly strain the system — from childhood trauma to sleep disruption, from loss to sudden success — and what research tells us about how they shape the course of bipolar disorder.