On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings

Photo: Loaded Landscapes
Even as I dedicate each of my blog series to a specific category of mental health (anxiety, bipolar, narcissism, ADHD, autism…), I’ve become familiar with a psychiatric sea change called transdiagnosis. This approach shifts from looking at each room in the house to looking at the house with all its rooms. This means in assessing, diagnosing, and treating an individual, a clinician looks across all the person’s symptoms and how they’re expressed, rather than how their characteristics or symptoms fall within bounds of a single, identifiable condition.
For people living with these diagnoses, this shift affects whether they’re told they have a mood disorder or a personality impairment, but rarely both — which in turn affects the focus of their therapy and/or medication. Not only that, it has an impact on how the person receives the diagnosis, and how society supports or stigmatizes that diagnosis.
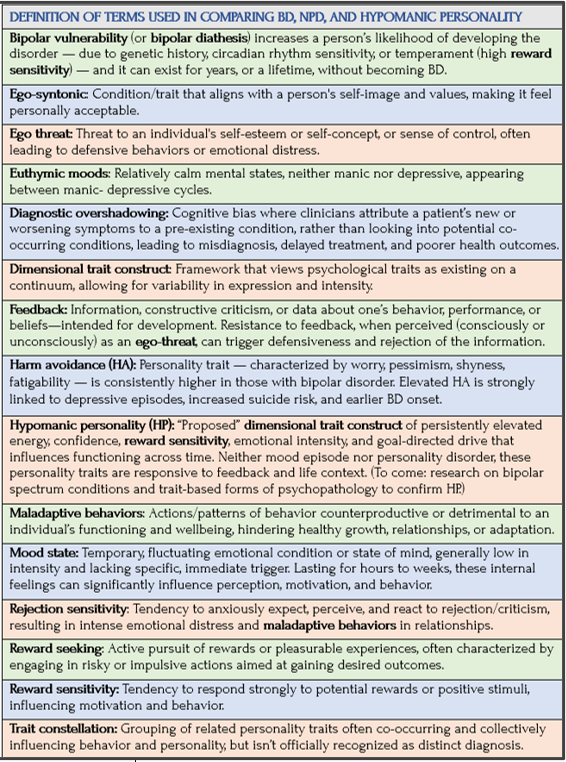
Dimensional Trait Constellations
To support this shift, an increasing number of new tests and frameworks can now assess former “disorders” as constellations or clusters of dimensional traits — that is, traits existing on a normality-to-psychopathology spectrum, rather than fitting neatly into discrete categories. This gives a picture of intensity, expression, “timing, persistence, flexibility, and relational impact,” as one researcher describes.
The American Psychiatric Association’s DSM-5 and its international cousin, the World Health Org’s ICD-10 (International Classification of Diseases and Related Health Problems, 10th revision) remain categorical systems. And yet, this broader shift toward transdiagnostic thinking is evident here as well, as both resources now incorporate more dimensional elements.
Two prominent transdiagnostic frameworks are the National Institute of Mental Health’s (NIMH’s) Research Domain Criteria (RDoC) and the Hierarchical Taxonomy of Psychopathology (HiTOP). They can determine what underlying processes may be responsible for comorbidity and symptom overlap between historically discrete disorders. So says psychiatrist and researcher Madeline Nagel in her thought-provoking review comparing bipolar disorder and narcissism.
The assumption of these dimensional models is that individuals diagnosed with the bipolar disorders or narcissistic personality disorder are at the extreme ends of these continua. Research results suggest both constructs are dimensional in nature rather than being discrete (taxonic) conditions….
Although the RDoC framework was proposed for research on psychopathology, it may call into question whether many DSM-5 or ICD-10 (WHO) diagnoses are useful fictions for conceptualizing and communicating about dysfunctional behavioral systems. —Madeline Nagel, PubMed/NIH
Consequently, Nagel writes, “qualitatively distinct conditions in DSM-5 may be at least somewhat similar when they are mapped onto these dimensional constructs. This suggests a possibility of shared or related etiologies [studies of the causes of medical/psychiatric illness].”
Here’s where I’ll leave RDoC and other frameworks, like the popular Five-Factor Model (FFM) of personality, which I define in the Glossary. The relevance for this post is to show how difficult it is to accurately assess and diagnose someone so they are effectively treated. Since bipolar disorder has a high rate of comorbidity, it’s unclear what guidance is available to clinicians to ensure the right treatment for their patients.
Diagnostic Overshadowing
Like jumping rocks to cross the stream, I’m hopping from term to term to make the case for what complicates diagnosis and gives rise to misdiagnosis — and thus inadequate or wrong care for those with bipolar disorder. Diagnostic overshadowing isn’t exactly saying my diagnosis is worse than yours, but close. Nagel notes how diagnoses can miss low levels of comorbidity because they don’t adequately identify people seen as having traits not captured by DSM-5 criteria. Here’s Nagel on why this suggests underestimating the prevalence of certain conditions.
Diagnostic overshadowing may also depress the number of people diagnosed with bipolar disorders and NPD. Individuals with comorbid BD and NPD are most likely to come to attention of clinicians during a severe mood episode. Thus, the focus would likely be on their mood symptoms and not on any longstanding personality features.
Meet Marcus: When Everything Looks Like Mood
Marcus, a 52-year-old Black man, is a sales manager currently on medical leave. Divorced and the father of two adult children, his relationships are strained to the breaking point. Tall, proud, impeccably dressed, Marcus has spent decades trying to conceal his mood swings. During hypomanic periods, his gestures are expansive and his charisma energizes the sales teams he leads. At the same time, he’s guarded and untrusting. His practiced confidence can read as arrogance, particularly in a workplace where vulnerability feels unsafe.
Marcus has long suspected he lives with bipolar disorder. His ex-wife once described him as “too intense,” a comment he dismissed as misunderstanding his ambition. Over time, however, untreated manic episodes made that intensity harder to deny. His family experienced him as entitled, dismissive, and emotionally unavailable, even when he saw himself as simply decisive.
Marcus finally enters treatment during a severe manic episode, triggered when his employer places him on medical leave. Coworkers had complained of being used, devalued, and ridiculed. A psychiatrist focuses — appropriately — on stabilizing his mood with medication.
As his mood improves, sleep normalizes and the most disruptive symptoms recede. Yet Marcus’s interpersonal patterns remain. He’s hypersensitive to criticism, feels deeply rejected by his children, and resents them for “misunderstanding” him. At work, he fears losing his job but struggles to see his own role in ongoing conflicts.
During follow-up visits, these patterns are attributed to “residual” bipolar symptoms, and treatment remains medication-focused. Marcus complies with medication but sees little reason to pursue therapy. Over time, progress stalls because enduring personality patterns are never named or addressed.
What began as a necessary focus on an acute mood episode becomes diagnostic overshadowing. Clinicians attend correctly to Marcus’s bipolar symptoms, yet miss the interpersonal traits that persist once mood stabilizes. Left unexamined, Marcus is haunted by an unspoken question: If this isn’t all bipolar, what does it mean for who I am? Without space to explore that question, treatment remains incomplete.
Bipolar Mood States, Hypomanic Personality, and Narcissism
Nagel picks up on Kay Redfield Jamison’s powerful 1996 book, Touched with Fire, and her profiles of artists with BD:

Richard Westall, Lord Byron (George Gordon Byron), (detail), 1813, National Portrait Gallery, London. Photo: The Art Newspaper
In her book on mood disorders and creativity … Jamison discussed a group of 18th-century poets who appeared to exhibit symptoms of mood disorders based on medical records, biographies, and other primary sources. The chapter on George Gordon Byron — commonly known as Lord Byron — argued that his famously impulsive, grandiose, hedonistic, appearance-obsessed, sensitive, and foul-tempered personality indicated that he likely had bipolar I disorder. Although Lord Byron appears to have had periods of both grandiosity and depression, biographical accounts of his life do not indicate an absence of grandiosity when he was not experiencing an “episode.” In fact, he is rarely described as anything other than pompous and self-important which may indicate that he had narcissistic personality features in addition to bipolar I disorder. The case of Lord Byron suggests the intriguing possibility that the bipolar disorders may have greater overlap with narcissism than is commonly recognized. —Madeline Nagel, from Kay Redfield Jamison, Touched with Fire
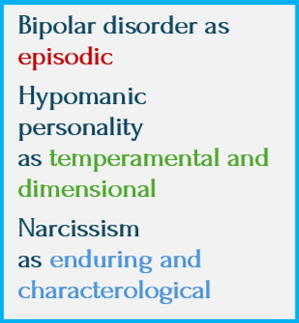
In this blog series, I’ve talked about how people with bipolar disorder (BD) can appear grandiose or unusually self-confident during manic or hypomanic episodes — expressing big ideas, bold aspirations, or over-confidence (especially when it comes to investing in sketchy deals). But here, I want to emphasize the episodic nature of this grandiosity and how it’s tied to mood states that typically lessen as mood stabilizes.
In the previous post, I described how people with a hypomanic personality are at risk for developing bipolar (most commonly BD-II). And some people with BD can also show a hypomanic personality.
It would be helpful to know this beforehand, because with the right care BD might go unexpressed for years – even a lifetime. Or the person with BD might get better, more targeted treatment for having both sets of traits.
Hypomanic personality can’t exist independently of bipolar vulnerability (diathesis) in someone who will never develop BD — even if that person’s mood instability stems from trait narcissism or other personality features. The key points here are:
- A hypomanic personality is not just a personality style.
- It’s best understood as a temperamental expression of bipolar vulnerability
- It isn’t a free-floating trait like extraversion, ambition, or emotional intensity.
Why the lines aren't always clear
Mental health diagnoses are often treated as distinct — you either “have” or “don’t have” bipolar disorder (BD) or a personality disorder (PD). Increasingly, however, research and clinical practice better understand many conditions as constellations of traits, rather than as sharply bounded categories.
In BD, some individuals show both episodic mood changes and stable temperamental traits — high energy, reward-seeking, confidence, and emotional intensity — that persist between mood episodes. This pattern is often called hypomanic personality: a temperamental expression of bipolar vulnerability resembling narcissistic traits in appearance, but not a fixed PD.
Trait overlap helps explain why similar behaviors may arise from very different underlying dynamics — and why careful attention to timing, persistence, and context matters more than labels alone. In this chart, I compare BP, hypomanic personality, and narcissism.
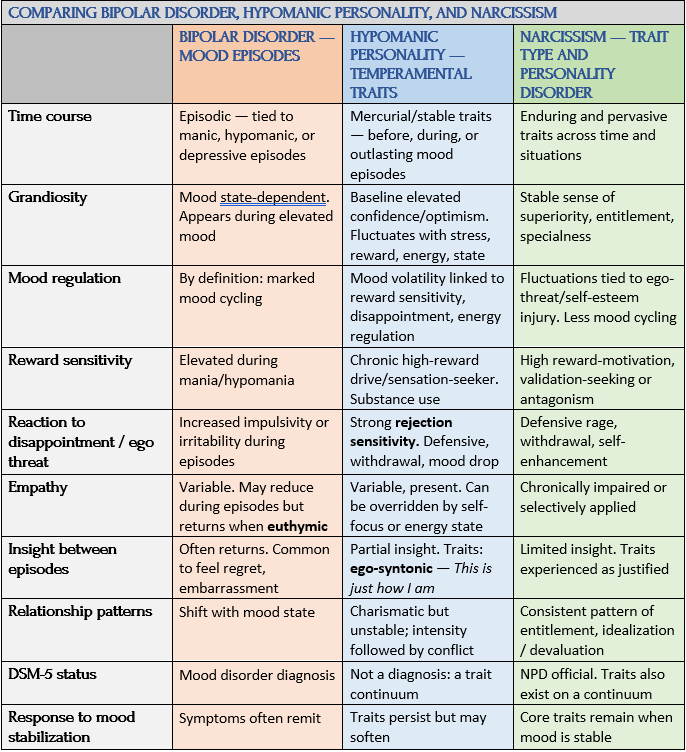
Source: Madeline Nagel, “Bipolar Disorders and Narcissism: Diagnostic Concerns, Conceptual Commonalities, and Potential Antecedents,” PubMed/NIH
Many people recognize these traits long before BD is a formal diagnosis — but as lifelong intensity, ambition, or emotional drive that felt normal or even adaptive until it tipped into impairment.
In contrast, narcissistic personality disorder (NPD) involves a pervasive and stable pattern of grandiosity, entitlement, and characteristic relational difficulties — resistant to feedback and not explained by mood shifts alone. In subclinical (unofficial, less severe) trait narcissism — specifically grandiose and vulnerable narcissism — stable personality characteristics tend to overshadow mood fluctuations, with diagnoses/treatment thus favoring narcissism over mood disorders. The converse is also true, as Nagel describes. A person in a manic phase of BD might not be treated for their personality features that remain once their mood lessens:
Whereas narcissism is considered to be a life-course, stable trait and the bipolar disorders are characterized by episodes of mania and depression, there is considerable research indicating that narcissism may be linked to mood instability (including depression) and bipolar disorder may have a pervasive personality component (i.e., hypomanic personality)….
[This] review examined the evidence linking narcissism and the bipolar disorders and suggests that considerable overlap may exist in the domains associated with reward- seeking, harm avoidance, and social functioning.
These comparisons show similar or overlapping traits — confidence, ambition, reward sensitivity, grandiosity, vulnerability — can arise from very different psychological dynamics. In BD, traits may appear episodically with mood shifts. In a hypomanic personality, traits may persist in a flexible pattern. And in narcissism, traits reflect a dimensionally rigid and pervasive personality structure.
Nagel’s research clearly supports a dimensional view of mental health. As she emphasizes in her work, “overlapping episodic mood symptoms, hypomanic personality traits, and fixed personality pathology can obscure meaningful differences …. From a dimensional perspective, it’s not simply which label applies, but how traits behave over time, how responsive they are to feedback, and how they shape relationships and daily functioning.” This dimensional view doesn’t mean personality disorders are less real — only that their features may share roots with other conditions.
Meet Elena: The Hypomanic Personality That’s Not a Phase
At 34, Elena is the very expressive embodiment of her Argentinian-American background — sharp eyes, quick smile, teasing talk punctuated by constant hand gestures. She works as a product designer at a startup, dressing creatively but professionally: structured jackets, bold earrings. In photos, she leans forward, animated, often mid-sentence. Friends describe her as “electric” — and, quietly, as “a lot.” Elena is close to her parents, not yet married, and very much wants children.
Since adolescence, Elena has been emotionally intense. She is ambitious, works obsessively, and takes pride in how far she’s come. She falls in love quickly, often with men who can’t meet her emotional depth. Even when she knows a relationship isn’t right, she feels profoundly wounded by rejection after breakups. The intensity exhausts her at times, but it also feels intrinsic — not a problem, just who she is.

Photo: iStock
Then something frightening happens. Elena stops sleeping and eating. She talks nonstop, grows suspicious, and alarms her friends. When they tell her she’s starting to sound paranoid, her mother brings her to a clinical care facility. She is diagnosed with a hypomanic episode and started on a mood stabilizer.
The medication helps — but once home, Elena feels unmoored. Her drive and confidence collapse. She becomes shaky and insecure, plagued by self-doubt and what feels like sudden imposter syndrome. At work, ordinary feedback now feels crushing, as though it carries too much weight. She struggles to understand why she feels so fragile.
Clinically, Elena did experience hypomania. But what remains is not ongoing hypomania, nor a personality disorder like borderline or narcissism. What Elena has is a hypomanic personality — a consistent pattern of temperament and drive that shaped her life long before diagnosis and persists outside of mood episodes. With an experienced therapist, Elena learns to recognize her hypomanic episodes in retrospect and how to work with her hypomanic personality rather than against it. In time, she can appreciate her creativity, idealism, deep relationships, and passion for life without being undone by them.
Further Research Needed
Comparing mood and personality disorders reflects a relatively new approach. But Nagel cautions that it’s still unclear how BD and narcissism are linked:
They may reflect different expressions of the same underlying tendency toward grandiosity and emotional vulnerability. In contrast, their associations may reflect a vicious cycle in which unstable mood states lead individuals to become more self-absorbed, or more self-focused beliefs cause emotional states to become magnified.
Nagel suggests seeing these two seemingly unrelated and contrary conditions on a continuum may result in fewer misdiagnoses, unnecessary self-blame, and stigma, and confusion — and can help individuals and clinicians focus on patterns that matter most for treatment, support, and long-term wellbeing.
Recognizing shared traits does not mean collapsing identities. Many people with bipolar disorder fear being seen as narcissistic when traits like confidence or intensity persist — yet flexibility, empathy, and responsiveness to feedback remain key differentiators.
In Sum: Uncertainty in What This All Means
What helps make sense of this trait overlap is that bipolar vulnerability, bipolar disorder, and narcissism can light up similar outward characteristics — confidence, intensity, ambition, social magnetism — but for very different reasons. In BD, this trait cluster can be driven by shifts in energy, reward sensitivity, and regulation. The bipolar “system” is amplified, not entitled. A person with BD can be carried forward by momentum, rather than the narcissist’s need for dominance or validation. In narcissism, the same traits spring from the need to protect self-esteem, personal narrative, and control of others.
The composite profiles in this post represent different clinical categories. In practice, they’re frequently the same person, encountered at different times in their lives.
These distinctions between temperament, mood vulnerability, and personality are commonly missed. Diagnostic error can cause years of misunderstanding, misdirected treatment, and unnecessary shame. This is real for too many people.
Here are questions to ask if any of this feels familiar:
- What patterns (thoughts, emotions, acts) repeat when your mood is stable?
- How do you respond to disappointment? To loss or rejection?
- Do your symptoms or traits feel less intense with feedback?
- Do such questions motivate you to find some answers?
The point of this post is to shift the question from “What kind of person am I?” to “What kind of underlying mechanisms are working in me?” I leave you with a prose poem that expresses these paradoxes and complexities:
Consequences by Jan Swan
Coming Up Next
In the next three posts, I begin a new sequence on diagnosis and system failure, from the difficulties at the institutional level to the personal one when acquiring a bipolar label. In Post 13: Bipolar Spectrum: Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma, I take on the issues of stigma and prejudice for those in need of healthcare, compassion, and understanding.