On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
8: Bipolar Disorder and Circadian Rhythms:
Why Sleep Isn’t Just Sleep — Part I

Circadian Rhythms
Many people with bipolar disorder can trace a manic or depressive episode back not to a thought or a feeling, but to days when they didn’t need sleep, didn’t eat, couldn’t tell if it was still morning, or drifted into nights without end. In these mood states, energy surged or receded, like ocean waves. They wondered what was happening or even whether they were imagining things.
Since my son Jaden was diagnosed with bipolar disorder (BD) some 13 years ago, I’ve been reading books and articles, listening to talks, and poking into research papers to understand his condition. So far bipolar is a mood disorder, a brain disease, a genetic condition affected by the environment, and a sleep disorder. None of this quite prepared me for the profound system called circadian rhythms — hiding in plain sight. There, but ignored, like breathing.
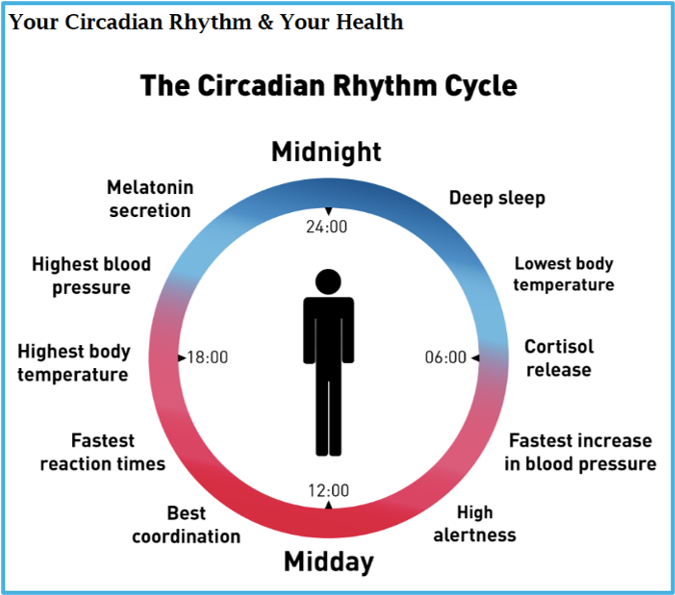
According to the National Sleep Foundation, circadian rhythms are driven by our body’s internal master clock, which helps control our sleep-wake cycle, eating habits and digestion, and body temperature. Usually it’s synchronized with the 24-hour day-night cycle. This biological process helps produce the hormone melatonin in the evening, causing that sleepy feeling, and gives us a dose of cortisol in the morning once light filters through the curtains, so we awake alert and ready for the day.
The National Institute of General Medical Sciences/NIH tells us circadian rhythms are physical, mental, and behavioral changes following this “about a day” cycle. But it can shorten or drift longer in some specific instances. Natural factors in our body produce circadian rhythms but signals in the environment, like daylight, as well as exercise and temperature, also affect them.
Source: NobelPrize.org
Problems occur when our biological clock doesn’t line up with the day-night cycle. Abnormal timing has been linked to health conditions like obesity, diabetes, sleep disorders, and mood disorders: seasonal affective disorder (SAD), major depressive disorder (MDD), and — the subject of this post — bipolar disorder (BD).
In this post I’ll give a flavor of the science behind our body’s miracle at the molecular level. And how genetic, biological, and life interference can destabilize cellular rhythms with dire consequences for those with heightened sensitivities. I’ll begin with some of professor Colleen McClung’s bulleted conclusions from her slide presentation:
- Bipolar disorder is associated with major disruptions to the circadian system.
- An altered circadian clock could be a causative factor in the disorder.
- Disruptions to normal sleep/wake schedules can precipitate episodes (particularly manic episodes).
- We are learning more about how circadian genes regulate dopamine and other brain functions that regulate mood.
Sleep and Reward as an Interacting System
Our brains, bodies, and energy systems run on daily rhythms that tell us when to sleep, wake, release hormones, think clearly, feel alert, be motivated, and recover from stress. When those rhythms weaken, change, or destabilize, our mood suffers.
Bipolar is a disorder of disturbed rhythms, with swings from mania (high energy, little sleep) to depression (low energy, over-sleeping) to euthymia (periods of relative stability).

What research is really saying is energy and activity changes are as central to bipolar disorder as mood changes.
This is a sea change in understanding — and in gaining psychiatric consensus. While formerly defined primarily by mood, modern criteria (DSM-5) recognize increased energy or activity is crucial to a BD diagnosis, often being a more defining feature in mania than just mood.
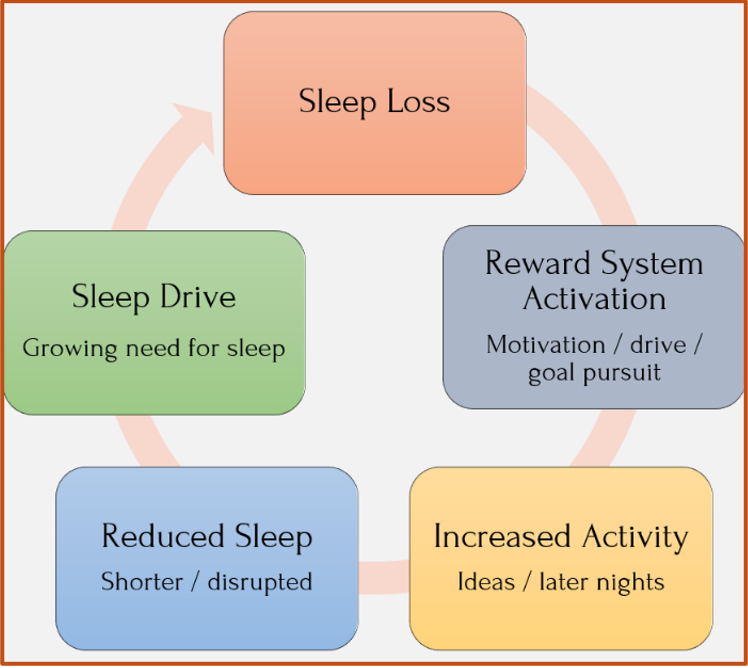
Sleep disruption can heighten reward-system activation — increasing energy, motivation, and goal pursuit — while reducing restorative sleep. As sleep debt grows, this feedback loop can intensify, making bipolar episodes more likely.
At the same time, sleep drive continues to build as a natural regulatory force. When in balance, the system can stabilize. But when activation outpaces regulation, the system can become a reinforcing cycle of increased activity and further sleep loss. In bipolar disorder, this can increase vulnerability to manic episodes.
Most of us have experienced circadian disruptions — notably jet lag, but also season changes, daylight savings time changes, blue-light exposure from our devices, or shift work — but nothing like the persistent challenges experienced by someone with a serious mental condition.
Evolution vs the Modern Era
In their paper, McClung and colleagues don’t spend a lot of time on how our circadian system evolved, except to say it brought our ancient forebears into the 24-hour cycle of daylight, darkness, and regularity. But it’s clear from the way modern life tampers with the natural ebb and flow of day and night that we evolved for world without lanterns and lightbulbs.
Modern life — artificial light at night and irregular schedules, often colliding within a single household — disrupts the brain’s timing signals.
How It All Works at the Molecular Level
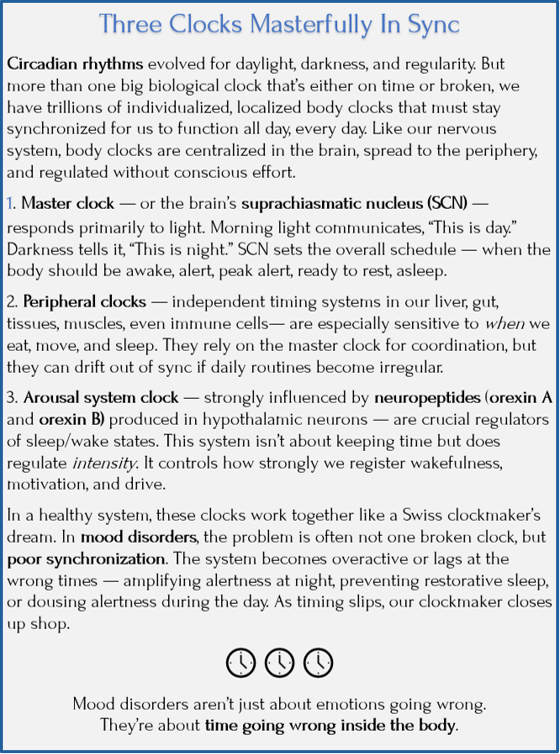
To understand why timing matters in mood disorders, we need to see how the brain keeps time in the first place. It does this through three tightly coordinated systems.
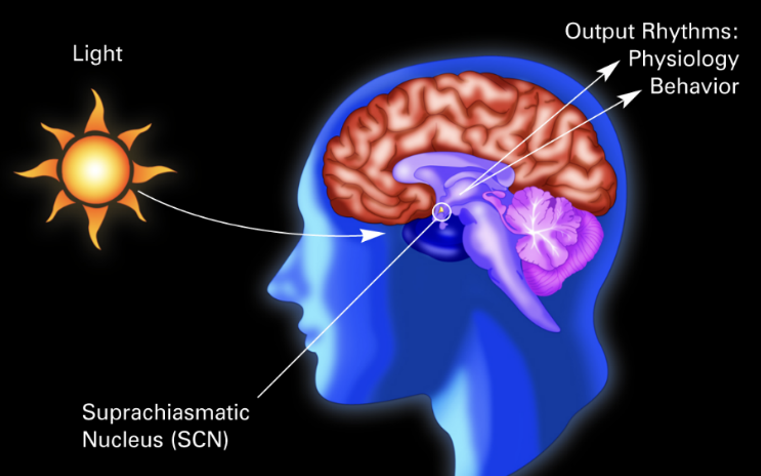
- The first is the suprachiasmatic nucleus (SCN), setting the overall schedule according to light.
- The second system is a molecular mechanism called the transcription–translation feedback loop (TTFL) that keeps the clock ticking.
- The third, a small but powerful signaling system built around orexin proteins, stabilizes the intensity of wakefulness within that schedule.
Here’s more on each of these systems:
Movement of proteins in a sleep-wake cycle. Colleen McClung, “Circadian Rhythms and Bipolar Disorder,” slide presentation for Brain & Behavior Research Foundation
System 1: The SCN
The Master Clock Sets the Schedule

The SCN, located deep in the brain’s hypothalamus, is the master clock – setting and coordinating time throughout the nervous system and into some organs (heart, liver) and tissues. It’s made up of a small cluster of neurons (nerve cells) that link light signals from our eyes to CLOCK genes inside our cells. This cellular activity is what aligns our body with the 24-hour day. Here’s the SCN’s unique role:
- Central coordination: Nearly every cell in the body has its own peripheral clock, but SCN is the primary coordinator.
- Direct light input: The SCN receives signals straight from the retina, allowing morning light to reset our internal clock to match the external world.
- Self-sustaining rhythm: Even in isolation, the SCN continues generating a near-24-hour rhythm. In transplant experiments, animals adopt the rhythm of a donor SCN — proof that this tiny structure sets the pace.
The SCN uses hormonal and neural signals to call time and regulate basic survival functions:
- Sleep–wake cycles: Signals darkness to trigger melatonin
- Hormones: Syncs the morning rise in cortisol with daytime alertness.
- Body temperature: Lowers core temperature at night to support deep sleep.
- Metabolism: Coordinates when the body is primed to use vs store energy.
Circadian misalignment results when the SCN falls out of sync, which over time has been linked to mood disorders, metabolic disruption, and cognitive changes.
The master clock in the suprachiasmatic nucleus (SCN), within the brain’s hypothalamus, is a tiny sliver of tissue as big as a grain of rice. SCN sits behind the optic nerve and tracks day and night from light entering the retina. It coordinates billions of miniature clocks — genes inside cells that switch on and off — in our physiological day. National Institute of General Medical Sciences/NIH
Pacemaker (Source) and Entrainment (Synchronization)
The SCN has also been called the master pacemaker that functions as an autonomous oscillator, generating the beat like a drummer in a band — if the drummer never stopped playing 24/7. The oscillator creates its own electrical signal without external input, dictating the tempo, driving organs to be rhythmic, and causing our brain to naturally feel sleepy just about every 24 hours.
Entrainment is the process of synchronizing these internal beats with an external signal (exogenous cue). Our environment adjusts the beat. In a research example, the SCN naturally ticks slightly longer than 24 hours. The morning sunlight “resets” or pulls it back to exactly 24 hours to match the world. Entrainment occurs when a dominant rhythmic system (the sun, a binaural beat, or another person’s speech) influences/stabilizes the pacemaker’s internal rhythm. Therapies using light can “tune” the metronome to match an outside rhythm, such as shifting sleep to a new time zone.
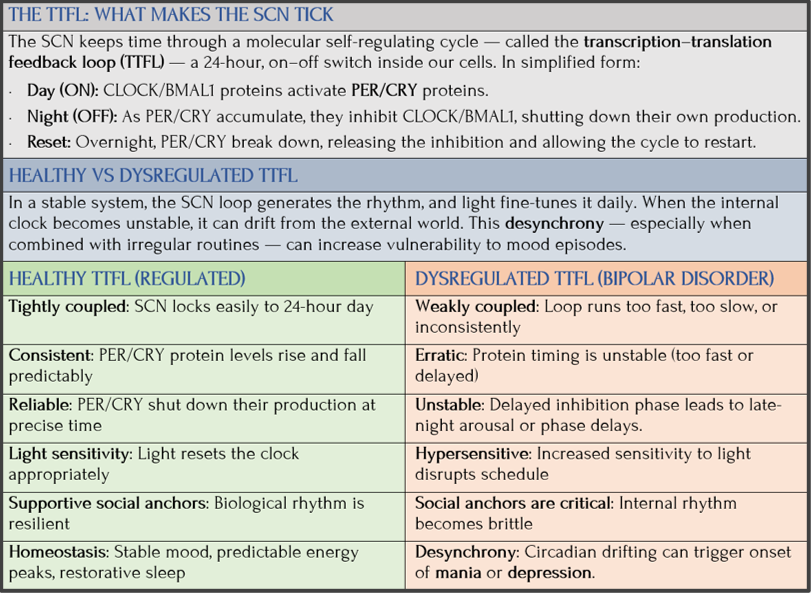
System 2: The Transcription–Translation Feedback Loop (TTFL)
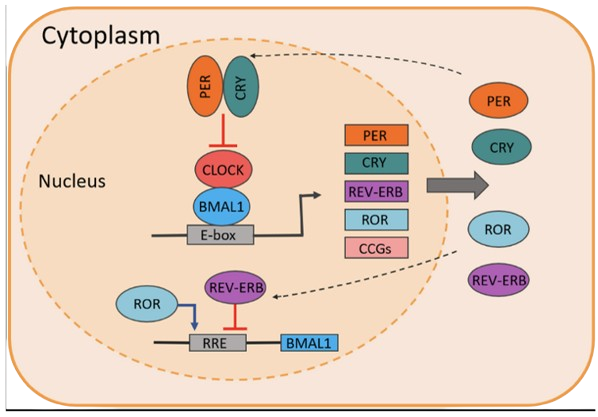
We also have complex molecular-level processes — the transcription–translation feedback loop (TTFL) — that generate the 24-hour rhythm. Scientists have discovered tiny proteins that move in and out of a cell’s nucleus in a process that turns day on and night off. It’s an ingenious system, but it too can go off.
In this chart, I give the briefest sense of this self-regulating loop and then compare healthy and bipolar versions.
System 3: Orexin
Orexin (also called hypocretin) stabilizes wakefulness within the SCN system. More to the point, it regulates the intensity of wakefulness — making sure we stay alert when the clock says we should be awake and engaged with the world.
- During the day, orexin levels rise to prevent unwanted sleep and support focus and motivation.
- When we’re stressed, excited, or hungry, orexin neurons fire more strongly, overriding sleep drive so we can respond.
- At night, orexin activity falls, allowing melatonin and GABA to quiet the system and permit sleep.
Orexin a and b are chemical messengers (a type of neurotransmitter called a neuropeptide) produced by neurons (in the hypothalamus) and these neurons release orexin throughout our nervous system. Out of billions of brain cells, only about 20,000 produce orexin — yet this tiny orexin factory has enormous influence over our daily functioning.
Without enough orexin, the boundaries between wake and dream states blur — as seen in narcolepsy, where most orexin-producing neurons are lost.
In Sum
Master clock SCN sets the timing, while peripheral clocks coordinate the body. TTFL ensures smooth timing at the molecular level, and orexin stabilizes wake intensity within that timing.
Rhythms are steady as long as these systems stay aligned. When they uncouple as in someone with bipolar, the result can be fragmented sleep, destabilized energy, and very vulnerable mood states. Here’s a way to illustrate our circadian rhythms:
Not Just Psychological, but Biological
Circadian rhythm research concludes mood episodes are not just triggered by stressors, no matter how severe they are. Just as likely, the body’s nervous system has lost its timing as its biological clocks fall out of sync. There are three biological processes that matter:

Mitochondria: Energy Timing
Mitochondria act like molecular power plants inside our energy-producing cells. The clock tells them when to ramp up energy production (usually during the day) and when to rest, ensuring we have energy when active and conserve it when sleeping.
In diabetes, the body may have the right key (insulin), but the lock on the cell won’t turn. A similar mismatch can occur in circadian dysfunction — even if we have plenty of fuel, we feel exhausted if these power plants aren’t coordinating their output to match what the body needs at that exact moment.
Dopamine: Mood/Drive Timing
Dopamine is such an important brain chemical for how we function that I’ve written about it in all my blog series. Both a neurotransmitter and a hormone, dopamine signals are linked to focus, motivation, reward, and knowing what’s important (salience). We think we need even more than our bodies produce to feel good, but the brain actually relies on precise timing. Dopamine signaling depends not just on amount, but on timing and pattern of release so the message doesn’t get scrambled and motivation doesn’t fade. The clock controls when this happens so we get the right message and feel the energy the mitochondria produces to do things during the day and then relax at night.
Metabolism Rhythm
Metabolism — the set of chemical processes that turn food into energy — means more than calories in/calories out. Our circadian rhythm controls the metabolism’s daily ups and downs, matching our energy usage to the time of day. We don’t burn fuel at the same rate all day. The clock dictates when our body is in “burn” mode (high metabolism) and when in “rest/repair.”
Ultimately, when these internal systems stop working together, we experience metabolic jet lag — the body’s machinery is present but it’s failing to work in harmony.
In Sum
Biological processes give rise to psychological outcomes, but it’s the mood disorder that gets noticed. Biological timing issues fly under the radar unless medical and psychiatric specialists are looking for it. Knowing this means there might be very different ways to think about what’s wrong.
Depression: Misaligned Mornings and Restless Nights
Multiple research studies agree that people exposed to more light at night have higher rates of depression and suicidal thoughts, including shift workers. And frequent long-distance travel can trigger depressive episodes, especially in people with a mental health history.
In her research, McClung adds further insights about the brains of people with depression, which her team found surprising. The normal daily rhythm of gene activity was “faded and disorganized.” And genes were out-of-sync with one another, especially in emotion-related brain regions. Even in primates, damaging the circadian system leads to poor sleep, anxiety, elevated stress hormones, and depressive behaviors.
This is how broken rhythms deepen depression:
- Stress hormones lose their rhythm: Cortisol normally peaks in the morning and tapers off. In depression, this rhythm often flips or flattens — leaving people tired in the morning and wired at night. This pattern increases vulnerability to future episodes.
- Immune system stays activated: Circadian disruption increases inflammation, which, in turn, further disrupts the clock. As sleep worsens, so does mood. The system gets stuck in a loop.
- Brain chemicals also lose timing: Just like dopamine described above, serotonin and norepinephrine need to be the right amounts AND the right timing. Disrupted light–dark cues cause these systems to falter, contributing to low mood and anxiety — even without obvious external sources of stress.
The Destabilizing Rhythms of Bipolar Disorder
This entire series has been about defining bipolar disorder subtypes — BD-I, BD-II, cyclothymia — according to the DSM-5 criteria for mood swings. But science knows this is equally about energy and timing swings. Our inner clock structures our daily routines: sleep, meals, social contact. ,When these clock settings or circadian cues get disrupted in vulnerable people, they cause biological rhythms to become unsteady, triggering mood episodes.
During mania, people feel wired, driven, and sleep very little. During depression, everything slows — including the body clock itself. It’s not just a feeling.
Biological rhythms can shift phase — advancing, delaying, or in severe cases losing stable entrainment to the 24-hour day — a phenomenon chronobiologist Franz Halberg described as “free-running.” As a result, both extreme moods can cause people to experience severely disrupted sleep–wake rhythms, extreme sensitivity to light at night, and evening chronotypes (I’ll get to this in the next post).
According to research, animals with damaged clock genes show behaviors that look uncannily like mania: hyperactivity, risk-taking, reduced need for sleep, and heightened reward seeking. Crucially, these behaviors emerge when activity happens at the wrong time of day. Timing matters as much as intensity. (Later, I’ll talk about how mood stabilizers like lithium reverse these effects — in part by strengthening circadian rhythms,)
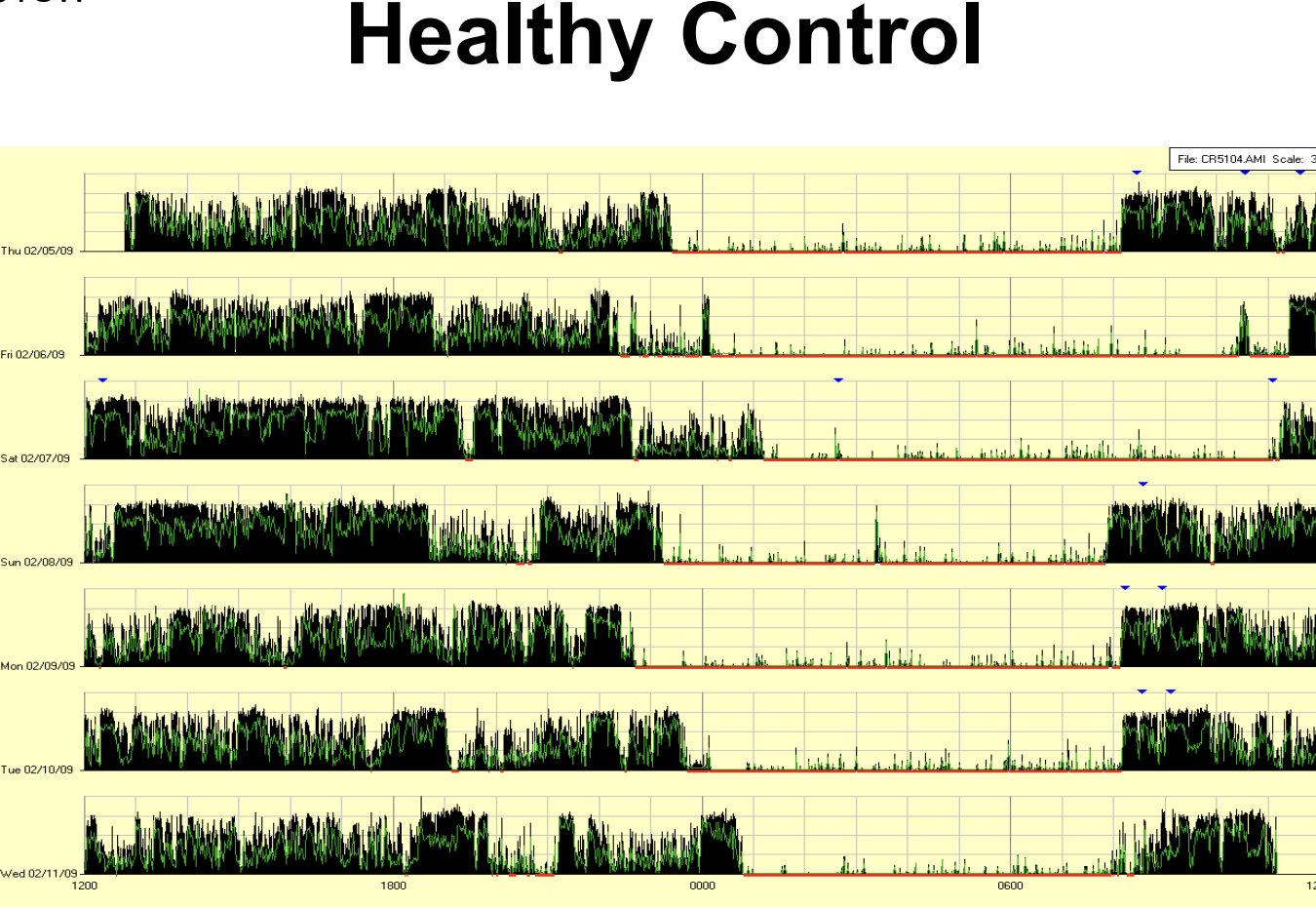
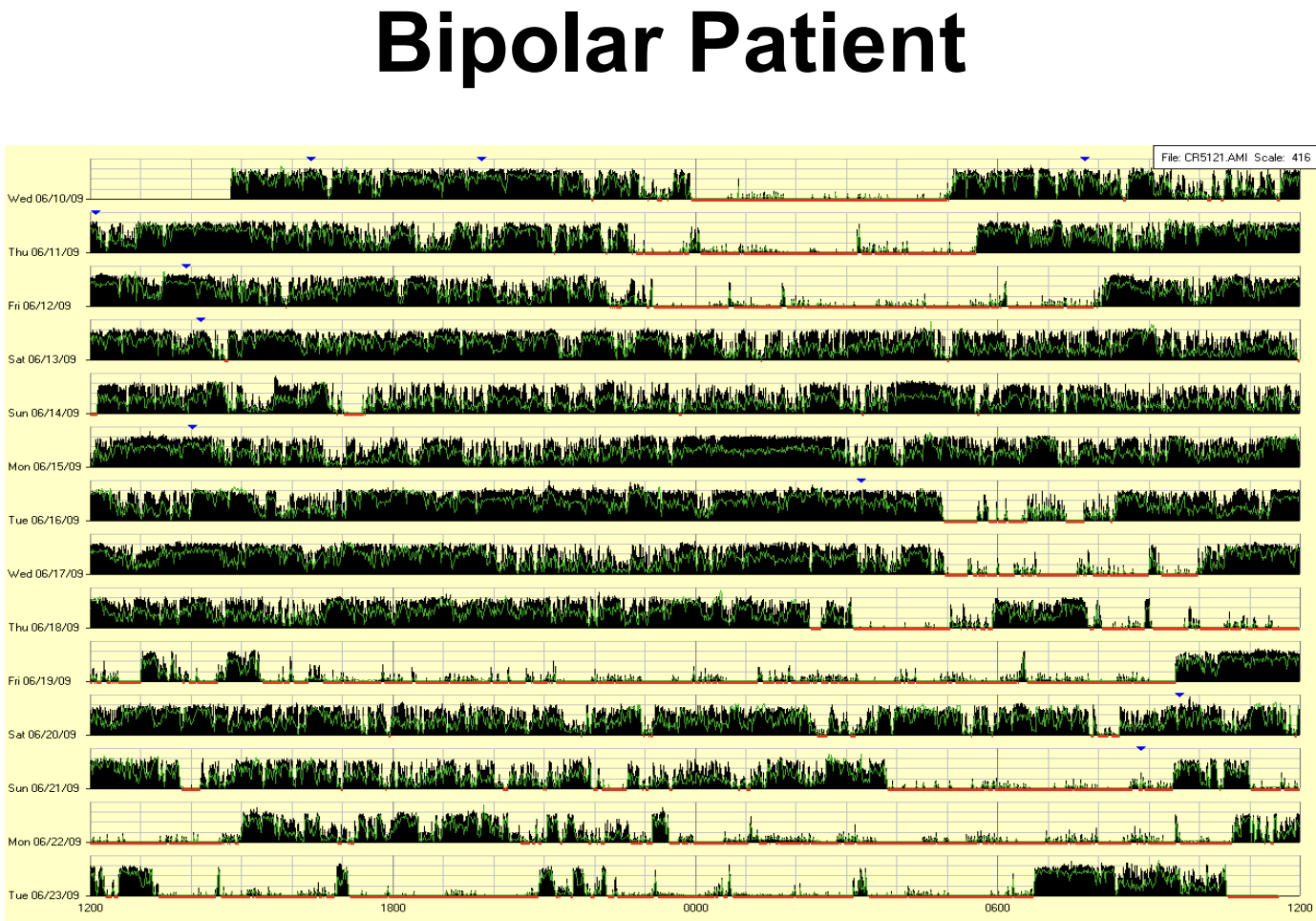
Comparing sleep/wake patterns of a healthy control with a bipolar patient. Colleen McClung, “Circadian Rhythms and Bipolar Disorder,” Brain & Behavior Research Foundation. Charts by Robert Gonzalez, MD, UTSW
Social Jet Lag: Circadian Misalignment
If someone told me a dozen years ago that bipolar disorder was less about emotional volatility than circadian rhythm vulnerability, I would have scratched my head in bewilderment. The simple fact is most people have a relatively steady internal clock and therefore don’t think about it unless they’re traveling across time zones. Most people with BD, however, deal frequently with their fragile internal clocks, their natural rhythms constantly shifting day by day and night by night, becoming erratic during extreme mood episodes.
Social jet lag is a persistent “geographical” mismatch between where our body is (home/work) and where its internal clock thinks it should be. It’s hard to forget that familiar Monday morning grogginess. Bipolar “Monday morning feelings” come more frequently and often more intensely, as the social/professional/financial demands of everyday life weigh more heavily.
One researcher noted by sleeping in on the weekends to catch up, we are effectively “flying” across four time zones back to work time. This constant resetting of the clock acts as a primary trigger for mood instability, turning a simple schedule mismatch into a much deeper state of internal chaos.
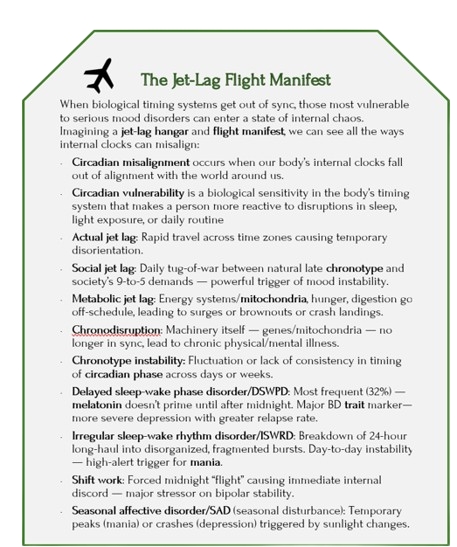
It was hard to remember all the timing functions/ dysfunction, so I created my own “jet-lag hangar” — with most of the ways they “manifest.”
Coming Up Next

Circadian research is accelerating, with increasing focus on precise, timing-based interventions — treatments that work with the body’s rhythms to align mood states day to day. The goal is not perfection, but steadiness: feeling sleepy before bed, refreshed after sleep, and alert at appropriate peak times.
Not only does this improve daily functioning, but it also reduces the frequency and intensity of mood disturbances.
Following these rhythms takes time and discipline — and it doesn’t erase loneliness or stress. Someone with bipolar disorder may still grieve the life they might have had, without strained relationships strained and lost opportunities. But this reframing, with guidance, can hopefully end blaming oneself and instead offer a stable foundation from which something lasting can be built.
In Post 9: Bipolar Disorder and Circadian Rhythms: Stability is the Goal — Part II, I describe our highly individual chronotypes and then describe promising treatments. While stability is the goal, protecting rhythm is the practice. Not a battle against oneself, but a gradual mind–body partnership — imperfect, ongoing, and real.
Sources
Listed at the end of post 9