On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
9: Bipolar Disorder and Circadian Rhythms:
Stability is the Goal — Part II

My two sons and I are all natural night owls. We might’ve thought this was our preference — or a bad habit. Well, it’s maybe both those things, but more importantly it’s how we’re biologically programmed. Our proclivity to stay up late and wake up late is innate. This is what science calls a late or “evening” chronotype. Despite the pressure of the traditional work or school day and feeling exhausted on a Monday morning, we become alert rather than sleepy at night as we should be heading for bed.
For my son Etan and me, you can attach insomnia to our chronotypes. For Jaden, with BD-I, I believe his sleeping patterns are irregular, have possibly moved off the 24-hour cycle, and sleep lengthens and shortens along with, and after, his mood episodes.
In fact, contrary to all good sleep hygiene, Jaden can miss midday sunlight entirely. For people like my son, their highly sensitive circadian systems do more damage than causing fatigue. They create a state of permanent biological mismatch with regular sleep-wake cycles.
Chronotypes and Circadian Phase Typing
Chronotypes are our body’s natural inclination to be awake or asleep at specific times. The concept was formalized in the 1970s through the Morningness–Eveningness Questionnaire by researchers Olov Östberg and James Horne. They confirmed what many of us intuitively know: some people are biologically early types, others late.
It’s called a type because — like blood or personality type — it remains relatively stable over long periods:
- Biological markers, tied to the SCN, vary by person (some have slightly shorter or longer than 24-hour cycles). Body temperature and alertness don’t peak until 6 pm. Melatonin (sleep hormone) starts rising around midnight.
- Predictability for when we have peak cortisol levels (for energy) or peak melatonin production (for sleep). If our job starts at 8 am, we’re forced to wake up right when our core body temperature is at its lowest point — when we’re biologically deadest to the world.
- Circadian gene variations, including PER3 and CLOCK, have been associated with both chronotype and bipolar vulnerability.
Phase Shifts in Different Sleep Cycles
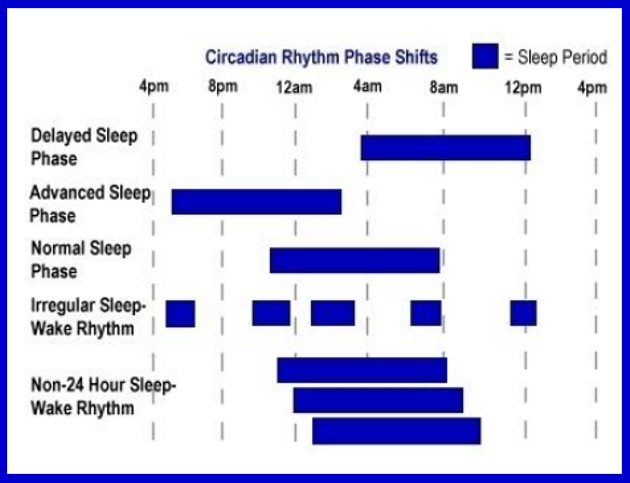
In “non-24 hour, sleep-wake rhythm,” three bars represent three sleep periods, each one shifting further away from the 24-hour cycle. Colleen McClung, slide presentation for Brain & Behavior Research Foundation
Bipolar’s Most Powerful Triggers: Changes in Sleep or Daily Routine
Chronotypes are increasingly seen as trait-like markers (endophenotypes) — determined by age and genetics, not personality. More than sleep, they dictate when our body temperature, hormones, and cognitive faculties peak throughout the day. People with BD are significantly more likely to be evening types than the general population. This biological phase delay creates a dangerous feedback loop with social jet lag, often worsening the course of the illness. Many studies corroborate these findings, leaving little doubt late night chronotypes correlate with mood disorders and to delayed melatonin onset. Yet, other studies suggest circadian phases may depend on mood state: circadian phase advance (mania) vs phase delay (bipolar depression).
Many with BD aren’t just wolves, but wolves whose clocks reset too easily or not at all. “Risk doesn’t come only from being a late chronotype, but from having a clock that is fragile, rigid, or slow to re-synchronize,” writes Michael Breus. Not all stabilization attempts work (“I tried to be a bear. It made me worse”). For some, forced early schedules increase stress, sleep deprivation, or mood instability.
four animal chronotypes representing human sleep/wake cycles.
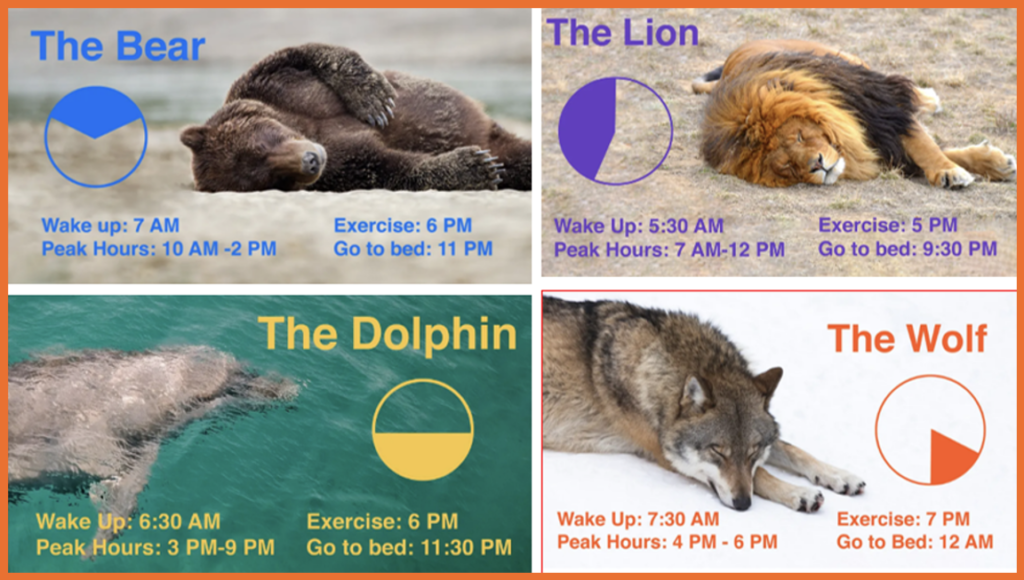
Popularized by clinical psychologist and “sleep doctor” Michael Breus, The Power of When. Graphics by Sarah Tew/CNET:
Bear (50% of people): Follows the sun, most productive 10 am–2 pm; sleeps well. Photo: Paul Souders/Getty
Lion (15%): Wakes up early with high energy but crashes by 9 pm. Best work before noon. Photo: JRL Photographer/Getty
Wolf (15%): Night owl. Struggles with early mornings; peak productivity starts after 6 pm. Photo: Anagramm/Getty
Dolphin (10%): Light sleeper. Often anxious, prone to insomnia; most alert late evening. Photo: S. Valeria/Getty
A Wolf Trying to Live Like a Bear
Diagnosed with bipolar II, Sally was a wolf by nature — alert late, creative after dark, slow to wake. She came alive at nights, mornings were tough as she scrambled to get her kids to school. She had to change. Life wanted her to be a bear: early rising, steady energy, predictable sleep. So she tried to become one.
Sally set earlier alarms, forced herself to earlier bedtimes, and pushed through morning with caffeine and grit. Sometimes it worked — briefly. She blamed herself for lacking discipline — it took so much out of her.
She slept more fitfully and didn’t have enough energy to see her through the day. She was frequently agitated, her thoughts racing, and she feared becoming destabilized. Her psychiatrist helped her see it wasn’t about trying harder. The shift came when Sally came to understand time.
Instead of forcing mornings, she protected them. She stuck to a realistic wake time that relied on light as good medicine, not punishment.

Image: Chat GPT
She took walks on sunny days, treated meals as anchors, and guarded evenings from overstimulation. Time spent winding down her young children for bed helped her wind down as well.
Sally never did become a bear. But, she stopped fighting her wolf nervous system.
The change was subtle but profound. Sally continued to experience mood episodes, but they became less frequent, less severe, and more understandable. She recognized what once felt like a personal failure at life was biological vulnerability — one that responded to self-care, not self-criticism.
For many people with bipolar disorder, stability doesn’t mean changing who you are. It means changing the conditions your internal clock lives in.
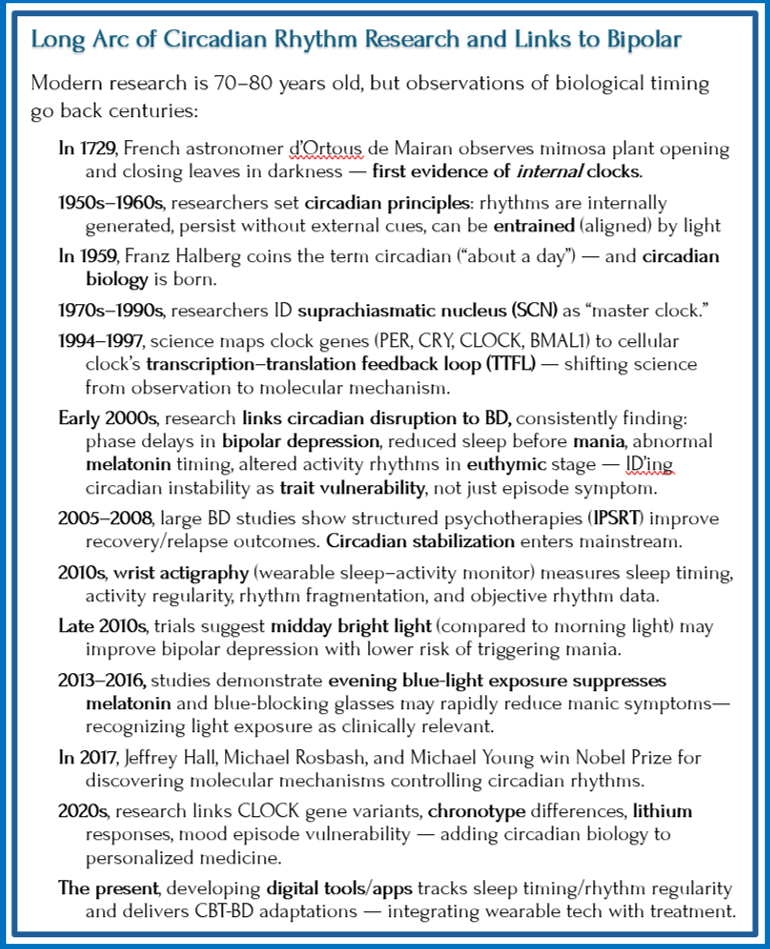
The next graphic summarizes research linking our biology to the sleep/wake cycle and, more recently, to bipolar:

Melatonin is Dusk, Cortisol is Dawn
Among the most studied circadian signals in bipolar disorder is melatonin — the hormone that tells the brain when darkness has begun. Released at night by the pineal gland under the direction of the brain’s master clock (the SCN), melatonin doesn’t shut us down, but makes it clear that night has arrived. It’s time to power down.
Cortisol works as its daytime counterpart. In the early morning, cortisol rises in what’s called the “cortisol awakening response,” helping us feel alert, mobilized, and ready to engage with the world. If melatonin is dusk, cortisol is dawn.
In bipolar disorder, these signals can lose their timing and precision. Melatonin may rise too late, too early, or fluctuate with mood state. Cortisol’s morning surge may be mistimed or feel blunted. As a result, a person with BD doesn’t only feel tired from poor sleep — they experience biological confusion. The body may feel alert when it should feel drowsy, wired when it should be winding down, depleted when it should be energized.
Some research suggests a circadian phase can shift in different directions depending on mood — advancing during mania, delaying during bipolar depression. Instead of a stable nightly rhythm, the darkness signal becomes reactive and fragile, overly sensitive to light at night, stress, or changes in routine. It’s at these moments when the internal clock can drift. For someone with BD whose system is already vulnerable, drift means destabilization.
Mismatches with the Environment
Some data suggest BD mood episodes are triggered by malfunctioning circadian rhythms interacting with external stimuli. Abnormal circadian rhythms are also thought to underlie sleep difficulties in BD. Here’s more data on all the ways this can show up:
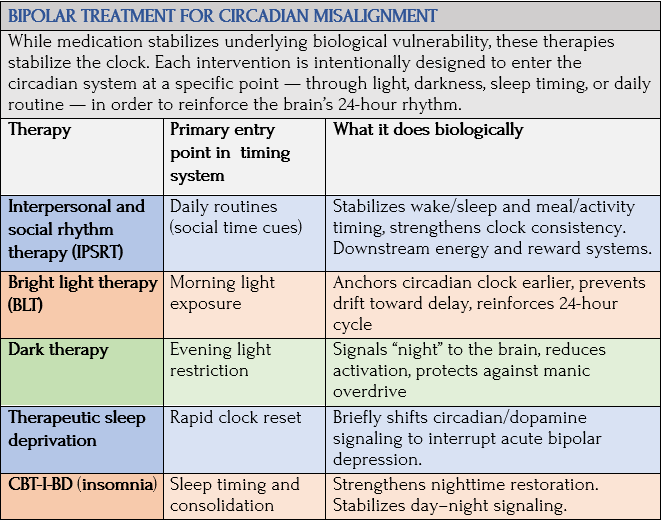
Bipolar Treatment: Anchoring the Shifting Clock

Image: Dreamstime
Understanding how BD is biologically tied to a fragile internal clock makes it clear why treatment isn’t about going to bed at a reasonable time. But it is about mechanical stability — preventing internal clocks from drifting away from the 24-hour sleep–wake cycle. By adopting specific therapies that reset the brain’s master clock, those with BD can help manually steady what biology is genetically and environmentally trying to disrupt. Here’s how we move from a jumping clock to a steady rhythm.
If we accept mood disorders being about nervous systems’ without a sense of time, then it makes sense that psychotherapies structured around time would help improve BD outcomes, along with medication. This is the case for those most frequently studied [additional BD treatments in post 17 and post 18]:
Interpersonal and Social Rhythm Therapy (IPSRT)
IPSRT believes extreme mood swings are often associated with relationship difficulties that lead to sleep deprivation. Grounded in social rhythm theory, IPSRT is based on this sequence: destabilized circadian rhythms disrupt daily routines that precipitate mood episodes in vulnerable individuals, which lead to sleep deprivation that hurt relationships.
According to the IPSRT website, the therapist helps the person with BD track sleep, wake times, meals, and social contact, working toward greater regularity while also addressing stressors in their relationships, difficult emotions (grief or anger), and changing roles. This — along with medication adherence — is essential to preventing relapse.
In randomized trials (particularly in BD-I), IPSRT is associated with longer periods of wellness, improved role functioning, and increased regularity of daily rhythms. Evidence is smaller in BD-II, but findings suggest meaningful improvements in depression.
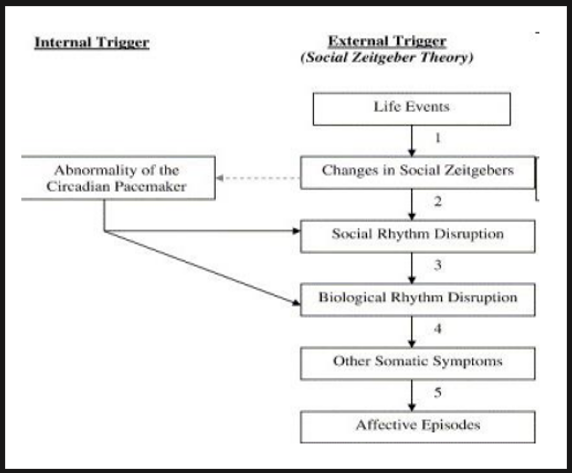
Theoretical Framework for Mood: To understand diagram, substitute “external social cue” for “zeitgeber.” Slide by Colleen McClung, Brain & Behavior Research Foundation
IPSRT is largely based on psychiatrist/ researcher Thomas Wehr’s 1990’s sleep studies that demonstrated how sensitive human biology is to light–dark exposure and small shifts in sleep timing — shifts that can destabilize vulnerable individuals. IPSRT mirrors Wehr’s findings by teaching people with BD that consistent periods of darkness and rest are neurochemical requirements for mood stability, rather than just going to bed.
The next chart shows relationship between unstable and stable sleep cycles with mood, in those with rapid-cycling BD:
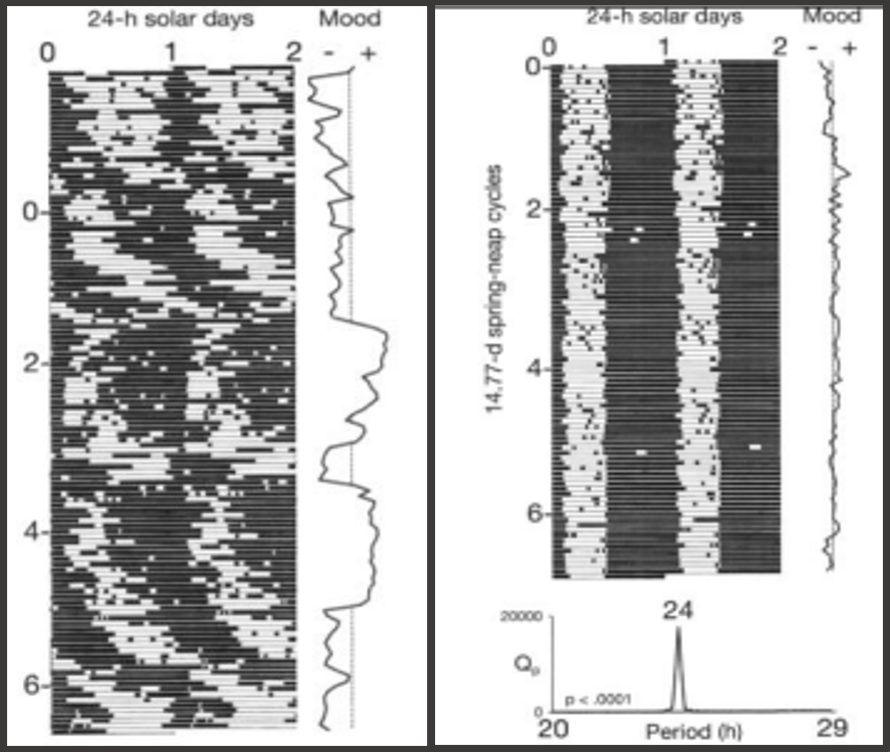
Actigraphy (wrist monitor) and mood data from person with rapid-cycling BD: Before and during a rigidly scheduled dark period.
L: Sleep–wake activity is fragmented and irregular across 24-hour days. Vertical line under “Mood” shows recurring oscillations — cycling between mood states in an unstable, repeating rhythm.
R: During strict nightly dark period, sleep–wake pattern consolidates into regular bands per 24-hour day. Under Mood, visible mood cycling largely disappears.
Comparison shows a core chronobiology claim: when environmental time cues (especially darkness) stabilize, circadian organization strengthens — and, here, mood cycling stops. Wehr et al., Translational Psychiatry, 2018, McClung slide presentation.
Bright Light, Dark Light, and Sleep Deprivation
Research highlights that controlling light exposure (maximizing natural light, minimizing night light) is a key, low-cost intervention for mental health. If mood disorders involve a timing problem, then treatment is about helping the body’s clocks run steadily and in sync — not just putting out emotional fires. There’s growing evidence that understanding a person’s individual circadian pattern could help predict which treatments will work best.
These methods work because they target what triggers bipolar, rather than only the symptoms (though they do that as well). According to McClung, et al., research emphasizes the need to integrate biological rhythms through the use of “advanced tools and mathematical models that can develop individualized ‘biological signatures’ for precise subtyping and personalized interventions.” McClung’s final two conclusions:
We are learning more about how mood stabilizing medications act on in the brain.
Stabilization and amplification of the circadian clock represents a therapeutic target for the treatment of bipolar disorder.
—Colleen McClung, slide presentation for Brain & Behavior Research Foundation
Light Therapies
Light therapy must be used cautiously — timing matters.
Bright light therapy (BLT) works differently for bipolar disorder than for depression or seasonal affective disorder (SAD). Where bright morning light effectively helps stabilize the circadian clock in unipolar mood disorders, in bipolar it can trigger mania for people with an overall greater sensitivity to light. So the best time to expose people with BD to light is mid-day (between 12:00 noon and 2:30 pm).
BLT uses a light box — emitting 7,000-10,000 lux of UV-filtered bright white light — placed on a table at eye level. (There are also head-mounted units or light visors.) Time required is 30 minutes–two hours/day.
Dark therapy (blue-blocking): During manic episodes, wearing amber-tinted glasses that block blue light in the evening can help dampen symptoms by simulating virtual darkness for the brain. Just as light therapy can improve mood, decreasing light can dampen manic symptoms.
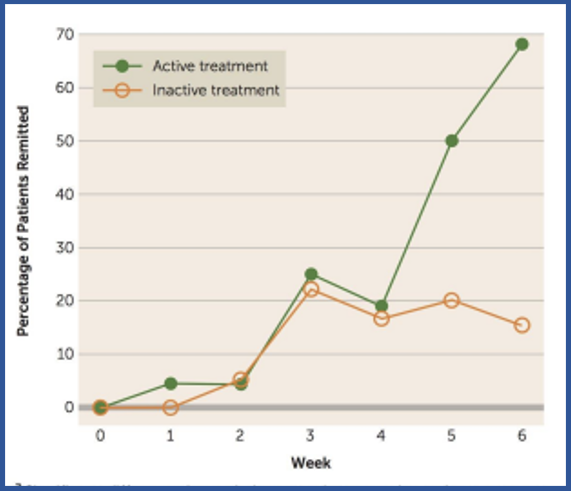
Midday Bright Light Therapy to Treat Bipolar Depression: Notable difference in treatment group remission rates over 6 weeks: active (68%) vs inactive (22%). Sit, Am J Psychiatry, 2013. Colleen McClung slides
Sleep deprivation therapy: Using sleep deprivation, a person is kept awake for 36 hours (total) or allowed to sleep for 4-5 hours/night (partial). Unfortunately, improvement in mood is short-lived. Sleep deprivation is only used during the depressive phase because it can provoke manic symptoms or worsen them.
IPSRT and light therapies are distinctive in placing the circadian system at the center of treatment, but it’s not the only path to stabilization. Other methods are CBT-I adapted for BD (CBT-I-BD), psychoeducation (not discussed here), and specific medications like lithium. Possibly even orexin modulation at some point.
CBT-I-BD
A form of cognitive behavioral therapy/CBT [see post 17], CBT-I-BD narrows its focus to sleep. It works by controlling or eliminating negative thoughts and actions that prevent sleep. Because insomnia and sleep irregularity are destabilizing, this adaptation accounts for bipolar risk. In controlled trials, CBT-I-BP has improved insomnia remission rates and, in some studies, reduced risk of mood relapse over follow-up periods. Sleep stabilization may also have positive downstream effects on mood stability.
In Sum
These treatments can be combined with each other and used with medications (mood stabilizers and antipsychotics). CBT-I-BD may allow a person to take a lower dose of an antipsychotic drug than would otherwise be needed to manage symptoms. Of course, using BLT in the evening may worsen insomnia, and dark therapy should not be used in depression.
Medication Advances
Bipolar medications will continue to be tailored to circadian rhythm stabilization.
Lithium / Valproate Therapy / SSRIs
Among common mood stabilizers, lithium [which I discuss in detail in post 15] has the strongest, long-term evidence for reducing relapse and lowering suicide risk. It works by affecting how cells send and receive signals along pathways, how circadian clock genes are expressed, and how mitochondria function. They appear to stabilize biological rhythms alongside mood.
Valproate (divalproex) is effective for acute mania, rapid cycling, and mixed states and is commonly used in maintenance therapy. While less studied than lithium, it seems to reduce mood episodes from recurring, but isn’t a strong antidepressant on its own.
Effective antidepressants (SSRIs) for major depression aren’t necessarily recommended for bipolar (see post 15), but can influence circadian timing indirectly by increasing serotonin availability. They aren’t considered rhythm-stabilizing agents in the way lithium or IPSRT are.
Melatonin / Agomelatine Therapy
Melatonin, released at night by the pineal gland (a small dark/light-responsive gland deep in the brain) is the body’s internally produced “darkness signal” that promotes sleep onset. Its strongest bipolar benefit is in correcting a delayed circadian phase and improving the quality of sleep.
Approved outside the U.S., agomelatine is an atypical antidepressant that acts on circadian phase via melatonin receptors and indirectly increases dopamine/ norepinephrine in the brain’s frontal regions (by blocking serotonin receptors). Evidence, which supports its efficacy in unipolar depression (with sleep normalization an added benefit), is more limited or mixed in treating bipolar depression.
Such melatonin-based therapies operate more directly on circadian alignment and sleep timing, but aren’t primary mood stabilizers. Some clinicians recommend melatonin supplements to help phase shift or reset the sleep-wake cycle, though evidence for its direct effectiveness in treating bipolar symptoms is still emerging.
Treatment Goal: Regulating the Biological Clock
The circadian clock regulates when mitochondria produce energy, when dopamine signals salience and motivation, and metabolism rises and falls across the day as it should. People evolved this way. The therapies I’ve explored here — rhythm stabilization, light and darkness interventions, sleep-focused treatments — differ from cognitive and emotional therapies. They aim to regulate the biological clock so that energy and reward systems activate at the right time. Psychosocial, pharmacological, and light-based approaches are promising avenues for treating and preventing bipolar mood swings. Bottom of Form
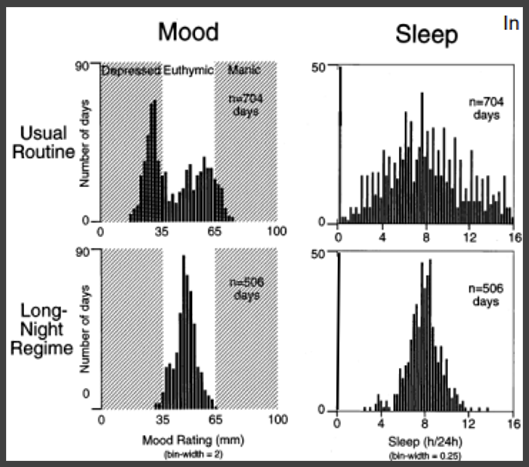
Treatment of Rapid-Cycling BD Patient: Use of long-night sleep to stabilize circadian timing.
Usual Routine: mood ratings span depressive-manic, shorter, irregular sleep. Long-Night Regime: mood ratings cluster in euthymic range, longer, consistent sleep.
Wehr, Sack, and Rosenthal, Archives of General Psychiatry, 1987), from McClung slide presentation.
Coming Up Next

It’s a tall order to comply with the rigor of a regular sleep-wake schedule for anyone, let alone someone with bipolar illness. I mentioned my research to my son Jaden and his first response was how hard this would be to do. He was interested but without breaking it down into guided steps in a therapeutic setting, I agree with him. The good news is understanding the science is a solid first step.
In Post 10: Reward Sensitivity and Bipolar Vulnerability, we re-encounter the word regulation, a word that signifies keeping our body systems stable and functional, not going off the deep end. I’ll show how bipolar disorder’s highly sensitized body systems can progress from a relatively stable and calm state to a mood episode.