On Bipolar Disorder
Show Table of Contents
INTRO
1. On Bipolar Disorder: Introduction
2. Jaden’s Story: A Journey to Mania
3. The Bipolar Rockies: A Witness to Mania
4. Bipolar Spectrum Disorder: More Than Mood Swings
5. How Bipolar Risk Takes Shape
6. A Sensitive System Under Stress
7. When Stress Accumulates
TIME
8. Bipolar Disorder and Circadian Rhythms: Why Sleep Isn’t Just Sleep — Part I
9. Bipolar Disorder and Circadian Rhythms: The Goal is Stabilization — Part II
SIGNIFICANCE AND MISREADING
10. Reward Sensitivity and Bipolar Vulnerability
11. Bipolar and Cannabis: Relief, Risk, and Regulation
12. Bipolar, Hypomanic Personality, and Narcissism: Similar Traits, Different Meanings
DIAGNOSIS AND SYSTEM FAILURE
13. Bipolar Diagnosis, Misdiagnosis, and the Hidden Barrier of Stigma
14. When Diagnoses Overlap: Bipolar, ADHD, Borderline
15. When Diagnoses Overlap: Physiological Drivers
16. The Raw Shock of a Bipolar Diagnosis
TREATMENT AND COPING
17. Bipolar Treatment: Medication Non-Optional
18. Bipolar Treatment: It Takes a Village
19. Coping With Bipolar: Things to Do
20. Famous People and Bipolar Disorder
21. Future Breakthroughs: New Bipolar Research
22. Bipolar Poetry: Inside My Mind
4. Bipolar Spectrum Disorder: More Than Mood Swings

Photo: Halo Effects
Bipolar disorder (BD) is a mental health condition characterized by extreme mood swings — from manic highs to depressive lows — in cycles of varying intensity and frequency. Previously called manic depression, BD has been recognized for thousands of years. Melancholia (depression) and mania are words from Ancient Greek. Ancient medical texts described how mineral salts sometimes calmed people suffering from mania and depression.
Today, lithium — a naturally occurring element found in some mineral salts — is one of the most effective medications for bipolar disorder.
In the mid-nineteenth century, French psychiatrist Jean-Pierre Falret described folie circulaire (circular insanity) in 1851 — widely considered the first clear clinical description of bipolar disorder.
In the early 1900s, German psychiatrist Emil Kraepelin analyzed the influence of biology on mental disorders, including BD. His work heavily influenced modern diagnostic systems.
Bipolar Disorder Types and Mood Episodes
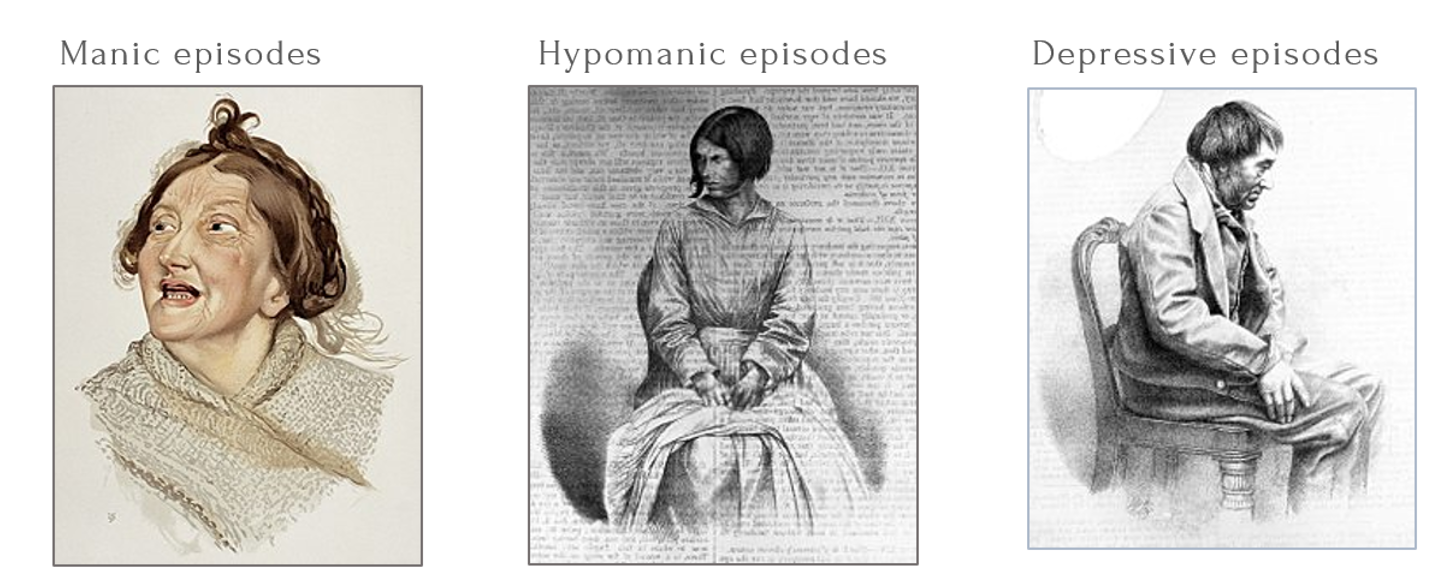
L-R: Woman Diagnosed with Hilarious Mania, 1892, color lithograph; Melancholy Passing into Mania, 1858, lithograph; Melancholy by William Bagg, after photograph by Hugh Welch Diamond
Bipolar disorder can disrupt nearly every part of daily life. It’s an illness with a strong genetic component that affects how people act, think, and feel. It can go unnoticed in quiet or down moments, but in elevated ones it roars to life. People can act in strange, undesirable, or harmful ways—mostly without recognizing the impact on themselves or on those around them. While close family, friends, or coworkers notice their behaviors as out of character and realize something is terribly wrong, they’re just not sure what or why.
The two main types are bipolar I and II — as referenced in DSM-5 — and both are characterized by mood swings. The difference is in the severity and intensity of mania. BD-I mania can become severe and may include psychotic symptoms in some cases. BD II mania, called hypomania, is less severe, its symptoms not lasting as long. The biological mechanisms that trigger BD’s high and low episodes are not well understood.
Mood Swings
Bipolar disorder’s core feature is dysregulated mood states, which cause difficulties with concentration, thought, energy, and behavior. They’re often accompanied by changes in sleep and eating patterns and can last for hours, days, weeks, and even months.
Although BD is distinctive from major depressive disorder (MDD), acute anxiety, or other serious conditions, it’s still frequently misdiagnosed. Here are the main mood classifications defining bipolar spectrum conditions:
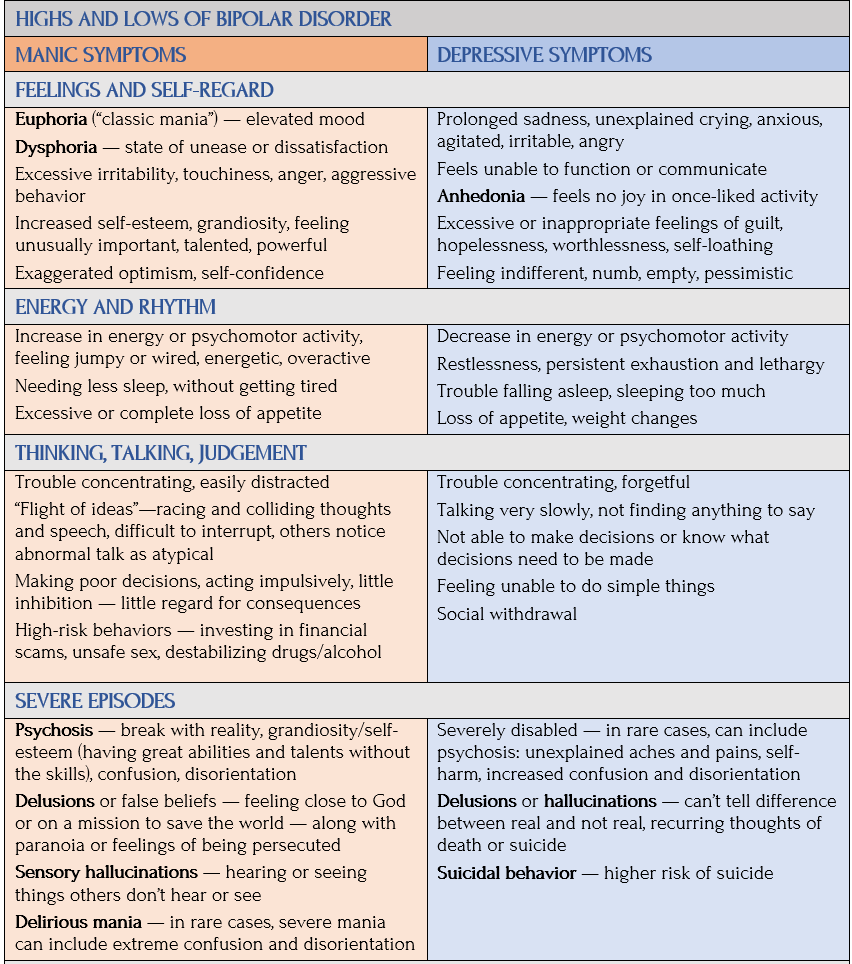
Manic Moods
During manic episodes, individuals may feel invincible, talk rapidly, and stay awake for days without feeling tired, often driven by an intense, restless energy that can lead to impulsive decisions. In fact, mania can move in different directions. One includes feelings of being super elated and euphoric. Another more irritable and hypersensitive.
Moods can turn quickly, becoming psychotic (no longer rational, with delusions and hallucinations).
Manic episodes have grace consequences — people think they can do anything they want, without regard, or perhaps disregard, for their behavior’s impact on themselves or anyone else.

Image: Generated by Leonardo.ai, Medium
Hypomanic Moods
Hypomania is similar — but less severe and destructive — to mania. It doesn’t lead to psychosis or hospitalization. Hypomanic behavior and activity can increase overall functioning, such as being hyper-focused and purposeful at work. But like the unpredictable course of its sicker sibling mania, it can also take a downward turn and have bad consequences for work or school, finances, and relationships. Often those in hypomanic phases deny anything is wrong when confronted about their behavior.
- Because hypomania can go unrecognized by healthcare professionals, it can be easily misdiagnosed as unipolar depression — another name for major depressive disorder (MDD) (see post 7 for more on misdiagnosis).
- Many with BD report hypomania as extremely stressful to live through. Without the correct diagnosis and treatment, people can go for years without correct medication. Sadly, this can also cause symptoms to get worse, resulting in more severe manic or depressive episodes.
Depressive Moods
The heavy burden of major depression, along with profound exhaustion and despair that can make routine tasks feel impossible, typically follows a manic or hypomanic episode — making it all the more difficult to withstand. BD depression ranges in feeling sad, empty, and hopeless to irritable, angry, and indifferent — without pleasure or interest in activities enjoyed when healthy (called anhedonia). Bipolar depressive episodes:
- Differ from regular mood fluctuations by intensity, lasting most of every day for at least two weeks and usually more.
- Last longer than manic episodes — and in some ways are more oppressive to live with than mania. Similarly to unipolar depression, a person can find it difficult to function, even to communicate, including with their spouse or partner.
Psychotic Episodes
According to NIMH, psychotic symptoms affect both thought and mood. Those experiencing psychosis may feel unstoppable, persecuted, or as if they have a special relationship with God, a great mission to accomplish, or other grandiose or delusional ideas.
Also called delirious mania, psychotic breaks with reality can include delusions (false beliefs, such as feeling connected to God or on a mission to save the world), visual and auditory hallucinations (experiencing things not there), confusion, paranoia, and feelings of being persecuted. Such episodes can:
- Can lead to severely impaired judgment or dangerous behavior.
- Result in either voluntary or involuntary admittance to an inpatient psychiatric hospital — depending on whether the person is a risk to themselves or to others or refuses treatment for behaviors noticed by others.
- Be associated with manic moods but can occur during severe depressive episodes.
- Be treated with anti-psychotic drugs that relax and slowly return the patient to “normal.”
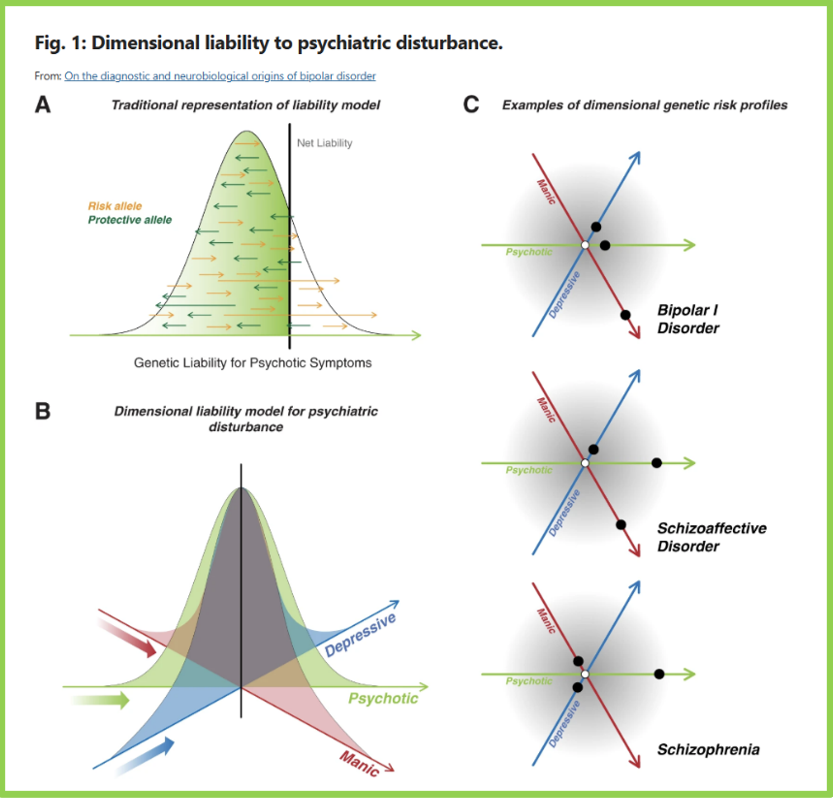
Models for how individuals fall along a spectrum of complex genetic risk for serious mental illness — here, psychotic symptoms. From Alexander Charn, et al., “On the diagnostic and neurobiological origins of bipolar disorder,” PubMed Central/NIH
Psychosis
Psychotic symptoms are most commonly seen in BD-I during manic episodes. Individuals may feel invincible, believe they’re famous, or act on dangerous delusions. In depressive episodes, they may experience paranoia, guilt, delusions, or hallucinations related to worthlessness.
In contrast, BD-II, characterized by hypomania, is less intense than full mania. Hypomania does not include psychosis. If psychotic symptoms occur, the episode is considered mania and the diagnosis shifts to BD-I.
According to doctor of nursing practice (DNP) Tanner Manwaring, “Bipolar Disorder and Psychosis: Understanding the Overlap,” Serenity Mental Health, psychosis may result from abnormal functioning in brain circuits, like those related to dopamine and glutamate regulation. Stress, trauma, sleep deprivation, and drug use can also trigger psychotic symptoms, particularly in those already vulnerable due to genetics or prior episodes.
Bipolar mania increases activity in certain brain regions, especially the prefrontal cortex and limbic system. This overactivation may disrupt reality processing. Early intervention is key.
Euthymic Moods
For all types and variations of bipolar disorder, there can be relatively stable periods between manic and depressive episodes. These between-episodes are called euthymia, but aren’t to be confused with remission. Mental health specialists use euthymia to establish a “baseline” of moods and behaviors — not only for bipolar but other cyclical mood disorders, such as MDD.
Bipolar Typology: Formally Diagnosable Subtypes
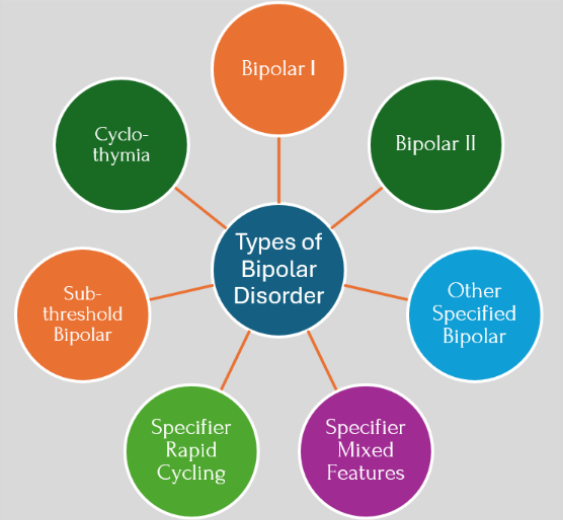
Types of Bipolar Disorder. Graphic: Jan Swan
The bipolar spectrum ranges from bipolar I (most severe) to bipolar II to cyclothymia subtypes, along with other variations in length, frequency, and patterns of manic and depressive episodes. To be diagnosed, individuals need to meet every DSM-5 requirement for an episode.
Bipolar I (BD-I)
The most severe subtype, BD-I can feel like a series of extreme shifts between two polarized worlds. At one end is mania, when the brain’s off-switch seems to disappear. At the other, is bipolar depression. Because BD-I requires at least one full manic episode lasting at least 7 days (or requiring hospitalization), the threshold for this diagnosis is defined by these intense extremes that significantly disrupt a person’s ability to function in their daily life.
Bipolar II (BD-II)
Diagnosis of BD-II requires at least one hypomanic episode lasting at least four days AND at least one major depressive episode. This alternating pattern is less extreme than BD-I, doesn’t end in psychosis, and rarely results in hospitalization.
Yet BD-II is hard to bear for the person who lives with it. According to Healthline, hypomania causes a surge in mood, energy, and drive, followed by deep depression and either feelings of dark despair or no feelings at all — just numbness.
With BD-II, people can be highly focused and purposeful, getting a lot accomplished and feeling great in the process. Or they can be and act desperately and destructively. Or both.
This can be hard on self-esteem. A person soars and feels capable of anything, and then crashes, feeling like a worthless failure. A difficult way to live.
Doctors often misread hypomania as self-destructive behavior, perhaps a substance abuse problem, or major depression or anxiety — all of which it can be, but it’s not the full picture.

Cyclothymia
Illustration: The Mighty
BD is typed as cyclothymia if recurring hypomanic and depressive symptoms are not intense or severe enough, or don’t last long enough, to qualify as BD-I or BD-II — nor are the depressive episodes severe enough to be diagnosed as major depressive disorder (MDD). For a diagnosis, cyclothymia episodes must alternate for at least 2 years, with symptoms lasting anywhere from hours to months — but never quite reaching the full severity of a manic or major depressive episode.
It also can include difficulties with concentration, thought, energy, and behavior; and with changes in sleep and eating patterns.
While cyclothymia is a formal diagnosis, it’s also a personality-level pattern that’s inherently subsyndromal — the highs include hypomanic symptoms but never meet the full criteria for a hypomanic episode. If they hit full peaks, the diagnosis upgrades to bipolar I or II. For at least two years, a person with this condition hardly feels “level,” but rather in a near-constant state of flux — up for a few days, down for a few days.
DSM-5 recognizes this state of near-constant flip-flopping causes clinical impairment and distress. Complicating the diagnosis, an individual may feel fine, be capable of handling daily life, and believe nothing is wrong — yet close family and friends recognize changes in mood or activity levels. There’s also a possibility of undiagnosed and untreated cyclothymia becoming more severe, turning into BD II.
Bipolar Spectrum Typology: Subthreshold Conditions
The term bipolar spectrum is used as an umbrella term to catch all the subtypes and subthreshold symptoms — that is, symptoms that don’t meet the full criteria for a formal disorder. Subthreshold specifically refers to fewer symptoms — such as symptom count or duration of mood cycles — even though the impact on the person can still be debilitating.
Other Specified Bipolar and Related Disorder (OSBARD)
Formerly called bipolar disorder-not otherwise specified (BP-NOS), this official bipolar diagnosis is now called other specified bipolar and related disorder (OSBARD). It’s used when a person has clear bipolar symptoms that cause significant distress or impairment, but which don’t meet the full, strict duration or symptom-count for BD-I, BD-II, or cyclothymia. A clinician might use this diagnosis if a patient has:
- Short-duration hypomanic episodes applies to individuals who experience hypomania, but for 2-3 days rather than the formal 4-day threshold. Despite the shorter timeframe, the episode must still represent a distinct change from the person’s usual behavior and be observable by others.
- Hypomania without depression: A history of hypomanic episodes but no major depressive episodes.
- Hypomanic with insufficient symptoms meets the 4-day duration requirement but exhibits fewer than 3 symptoms (or 4 if the mood is irritable) required for a full diagnosis. A person might experience elevated mood and increased energy but lack other symptoms (like pressured speech or grandiosity) needed to cross the threshold.
- At-risk/prodromal features are “pre-threshold” behaviors often seen in adolescents or young adults. This may include cyclothymic temperament (habitual, rapid mood swings that are part of the person’s personality), unexplained irritability, and micro-episodes of high energy lasting only a few hours. While not yet a disorder, these features are statistically linked to the future development of formal bipolar episodes.
Subthreshold Bipolar
This is a more general term often used in research and clinical discussions to describe the soft end of the bipolar spectrum. It refers specifically to the presence of manic or hypomanic symptoms that fall below the threshold of a standard diagnosis. It most often describes people who have recurrent subthreshold hypomania (brief or mild ups) alongside major depression. Research suggests that many people with subthreshold symptoms may eventually develop full BD, making it an important category for early monitoring.
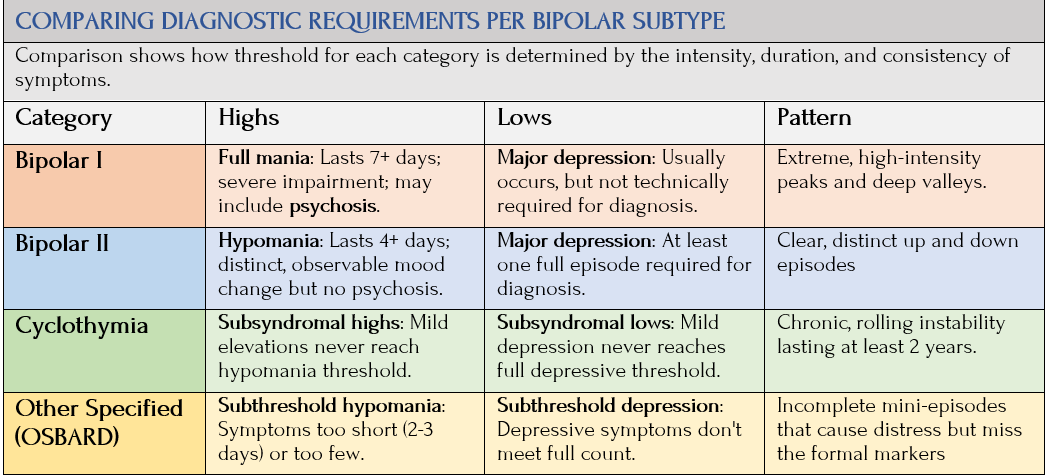
The following chart compares the threshold range of symptoms for each bipolar subtype:
The Specifiers: Mixed Features and Rapid Cycling
In the past, mental health professionals treated mixed features and rapid cycling as separate bipolar categories, but now they call them specifiers, which act as tags added to a bipolar diagnosis to describe how its currently behaving.
Mixed Features

To be diagnosed with the rapid cycling specifier, a person would need to experience at least four alternating episodes of mania, hypomania, and depression in a 12-month period. Stable periods (euthymia) occur between the episodes.
Rapid cycling can occur with any BD type and may be a temporary condition, occurring at different times in one’s life. More research is needed about causes, diagnoses, and treatment.
Why do these distinctions matter?
Understanding specifiers vs types helps professionals to target treatment. One doesn’t tend to be diagnosed as bipolar, but maybe as bipolar II, currently experiencing mixed features. That might explain why a person feels “tired but wired” or why their mood feels so unpredictable. It validates the reality and distress of subthreshold symptoms.
Remission and Recovery
Since bipolar is a chronic, lifelong condition, there isn’t a cure — so remission is the primary goal of treatment. It means symptoms have reached a point where they no longer interfere with daily life. Clinicians categorize two types:
- Full remission is the complete absence of mood episodes for typically at least eight consecutive weeks, with mood returning to baseline.
- Partial remission is no longer meeting the full criteria for a mood episode, but some mild, lingering symptoms remain, like slight sleep disturbances or mild low energy.
Studies suggest roughly a third of people with bipolar disorder experience extended periods of remission. While remission can last for months or even years, the risk of relapse remains — often triggered by stress, sleep loss, or stopping medication — requiring long-term management to maintain this state.
Recovery is often used to describe a broader state where a person has both stable moods and has fully restored their ability to work and maintain a social life. About 23% of people diagnosed with BD achieve complete mental health — being free of all psychiatric disorders and substance abuse for at least one year, while reporting high levels of happiness and life satisfaction.
About 35% reach functional recovery by an ability to work and live independently. This is harder to achieve than symptom remission. Studies show, even when symptoms disappear, many people still struggle with professional or social impairment.
Bipolar At-A-Glance
Coming Up Next

The next posts cover risk factors (causes), symptoms, diagnoses, and treatments. In posts 5-7, I’ll move from familiar bipolar terrain of typing and mood swings to what goes on beneath all that to understand the vulnerability and stress that create bipolar risk — stemming from genetic, biological, and environmental factors. In BD, repeated stress can gradually change how the brain regulates mood and energy, making it easier for manic states to emerge even without new genetic factors. A person’s life circumstances are so individualized, which makes the onset of this illness, across cultures, time, and history, even more remarkable and so confounding. I’ll begin with Post 5: How Bipolar Risk Takes Shape, where risk isn’t about danger but about all the layering of risk factors that accumulate to trigger a sudden and devastating bipolar episode.
Sources